Access to Medicine Index
The Access to Medicine Index is an independent initiative that ranks the world’s 20 largest research-based pharmaceutical companies according to their efforts to improve access to medicine in 107 low- to middle-income countries.[1] The Index assesses how companies are making their products more available, affordable, accessible and acceptable to patients in need. By comparing companies to one another, the Index aims to stimulate pharmaceutical companies to play a bigger part in addressing the challenges of access to medicine in developing countries and to offer them insight into the activities of their peers.[2][3] Furthermore, the Access to Medicine Index seeks to create a platform for stakeholders from the pharmaceutical industry, governments, investors, civil society, patient organisations and academia to gather and form a common view of how these pharmaceutical companies can make further progress.
The Access to Medicine Index is published every two years by the Access to Medicine Foundation, an international not-for-profit organisation dedicated to improving access to medicine for people in need. The organisation is based in Haarlem, The Netherlands and receives financial support from donors such as the Bill & Melinda Gates Foundation, the UK Department for International Development (DFID) and the Dutch Ministry of Foreign Affairs.[4]
The most recent Access to Medicine Index, published in November 2016, ranks the top 20 pharmaceutical companies as follows:[5]
| Company name (2016 score) | 2016 Ranking | 2014 Ranking |
|---|---|---|
| GlaxoSmithKline (3.43) | 1 | 1 |
| Johnson & Johnson (2.93) | 2 | 3 |
| Novartis (2.87) | 3 | 4 |
| Merck KGaA (2.83) | 4 | 6 |
| Merck & Co. (2.65) | 5 | 7 |
| Sanofi (2.58) | 6 | 8 |
| AstraZeneca (2.53) | 7 | 15 |
| Gilead Sciences (2.45) | 8 | 5 |
| AbbVie (2.39) | 9 | 9 |
| Novo Nordisk (2.35) | 10 | 2 |
| Eisai (2.34) | 11 | 11 |
| Bayer (2.03) | 12 | 10 |
| Bristol-Myers Squibb (1.97) | 13 | 13 |
| Pfizer (1.87) | 14 | 16 |
| Takeda Pharmaceutical Company (1.77) | 15 | 20 |
| Boehringer Ingelheim (1.70) | 16 | 14 |
| Eli Lilly (1.67) | 17 | 17 |
| Daiichi Sankyo (1.61) | 18 | 19 |
| Roche Holding (1.36) | 19 | 12 |
| Astellas Pharma (1.32) | 20 | 18 |
History
The Access to Medicine Index was developed starting in 2004 on the initiative of Dutch entrepreneur Wim Leereveld.[6] After years of working with the pharmaceutical industry, he concluded that simply "naming and shaming" the industry did not do enough to encourage pharmaceutical companies to play their part in improving access to medicine in the developing world. Leereveld noticed that there were many different (and sometimes conflicting) opinions about what the pharmaceutical industry should be doing with regard to access to medicine, but that there was no tool to recognise good practice within the pharmaceutical industry and no framework for collective dialogue surrounding this issue. He set out to develop a ranking system that would show which pharmaceutical companies do the most to improve access to medicine and how, and also help stakeholders to collectively define companies’ role in increasing access to medicine.[6]
The first Access to Medicine Index was published in 2008, followed by a new Index every two years.
Methodology
The 2015 Methodology for the 2016 Access to Medicine Index was published in October 2015.[1]
The Access to Medicine Index uses a weighted analytical framework to capture and compare company data. The framework is constructed along seven areas of focus called ‘Technical Areas’, which cover the range of company business activities considered relevant to access to medicine. Within each area, the Index assesses four aspects of company action called ‘Strategic Pillars’: commitments, transparency, performance and innovation.[1]
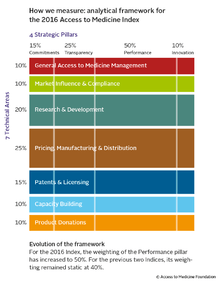
Technical Areas[1]
General Access to Medicine Management: This Technical Area investigates how companies integrate access-to-medicine issues within their corporate strategies, governance structures and management systems. It analyses how companies engage with stakeholders, consider their stakeholders when making plans and are transparent about stakeholder engagement activities. The Index also examines the strategic rationale behind companies’ access strategies.
Market Influence & Compliance: This Technical Area looks at how companies interact with (or finance) external organisations, such as governments, patient groups, and think tanks, and where these links may affect access to medicine by influencing policy. It also examines evidence of breaches of ethical marketing codes, corruption and bribery, and how companies mitigate the risks of breaches occurring.
Research & Development: This Technical Area analyses in-house and collaborative R&D efforts aimed at developing new or adapted products for diseases within the Index scope. It also examines whether companies put steps in place during development to accelerate and facilitate access to products for people living in low- and middle-income countries on market entry. The Index also investigates companies’ clinical trial codes of conduct, evidence of oversight and enforcement mechanisms for these codes, and whether there is evidence of breaches of clinical trial conduct in countries within the Index scope. Finally, it examines the transparency of data surrounding companies’ clinical trials, such as the publication of trial results (whether positive or negative) and the sharing of patient-level clinical trial data with trusted external parties.
Pricing, Manufacturing & Distribution: This Technical Area centres on how companies take affordability and other socio-economic factors into account when developing pricing strategies, and how their manufacturing and distribution practices ensure products are available, affordable and used appropriately, and that their quality is not compromised.
Patents & Licensing: This Technical Area looks at how companies support a healthy, competitive market for pharmaceuticals. This includes managing the impact of patent monopolies on medicine prices (e.g., by taking steps that support both the market entry of generic medicine manufacturers, and the activities of drug procurement agencies), and by refraining from anti-competitive activity.
Capacity Building: This Technical Area seeks to capture the long-term, systematic engagement of companies with local stakeholders to build local capacities for providing healthcare. It examines how companies contribute to the strengthening of local research, development, production and distribution systems, and how they support the skills and knowledge of people needed to keep these systems functioning. It also looks at how companies help build national systems for monitoring product safety once products reach the market.
Product Donations: This Technical Area looks at companies’ product donation programmes in countries within the scope of the Index. It examines how companies partner with external organisations such as governments and local NGOs in order to ensure much-needed medicine reaches patients living in the intended communities.
Methodology development [1]
The Access to Medicine Index methodology is developed in consultation with many individuals and organisations around the world. The stakeholder consultation and review process occurs every two years, starting in the year prior to the publication of an Index. This process is meant to keep the Access to Medicine Index responsive to the changing global health environment, based on expertise from a broad range of relevant perspectives, and to enable refinement of the framework through which companies are assessed.
As a first step, the Access to Medicine Foundation’s research team assesses the quality and robustness of each indicator using quantitative tests. The Foundation then consults with experts to update the methodology and to build consensus regarding the appropriate role for pharmaceutical companies in addressing access to medicine. The Foundation also reviews the previous Index with the companies that are measured. Throughout the methodology review, formal committees provide support to the Index team, including strategic guidance from the Expert Review Committee (ERC). The ERC also ratifies the methodology prior to publication. The details of the process vary depending on the evolving needs of the initiative.
The ERC is made up of individuals from a variety of stakeholder groups all active in some capacity on the access to medicine agenda. The mandate of the ERC is advisory in nature with the objective of providing guidance, recommendations and advice to the Access to Medicine Index team on the scope, structure, content and methodology of the Access to Medicine Index assessment. The diverse composition of the ERC is meant to ensure different viewpoints and perspectives are taken into consideration when establishing the latest Access to Medicine Index Methodology.
Data collection
Once the methodology has been agreed upon, the Access to Medicine Foundation collects and analyses company data. Data for the Access to Medicine Index comes from a variety of sources, including publicly available material, information provided by companies via an online platform and information sent from other bodies to those developing the Index upon request.
Scoring[7]
In accordance with the Access to Medicine Index methodology framework, companies measured by the Index receive a separate score for each Technical Area. These scores are composed of multiple indicator scores that measure a company’s commitment, transparency, performance and innovation within each Technical Area. A company’s overall score, which determines its overall Index rank, is a weighted combination of its scores in each Technical Area. Company scores are calculated on a relative scale of 0 to 5, with 0 indicating the lowest score among the company set and 5 signifying the highest score among the company set.
Scope
Company Scope[1][8][9][10][11]
The Access to Medicine Index ranks 20 of the world's largest originator (research-based) pharmaceutical companies, based on market capitalisation and the relevance of their product portfolios to diseases in the developing world. One unlisted company, Boehringer Ingelheim, is also included since it meets the size and portfolio relevance criteria.
In 2008 and 2010, the Access to Medicine Index also measured companies engaged exclusively in the production of generic medicines. Based on feedback from the 2011 stakeholder consultations, these companies were excluded from the 2012 Index and subsequent iterations. The Access to Medicine Foundation states that it recognises that these companies play a significant role in access to medicine, particularly in low- and middle-income countries.
Geographic scope[1]
The Access to Medicine Index focuses on low- and middle-income countries, based on World Bank[12] and United Nations[13] classifications measuring economic advancement, human development, and relative levels of inequality. The 2016 Index measures developments in a total of 107 countries.
The 2016 Index includes countries that are considered to be low income and lower-middle income countries by the World Bank, and Least Developed Countries (as defined by the United Nations Economic and Social Council).[14] In addition, countries that are classified as low human development countries and medium human development countries by the UN Human Development Index are included. Finally, based on the UN Inequality-Adjusted Human Development Index, the Index includes countries which, while they may have higher measures of development, have comparatively high levels of socio-economic inequality.
Disease scope[1]
The Access to Medicine Index covers a range of diseases based on their aggregate global disease burden and their relevance to pharmaceutical interventions, in accordance with non-age-weighted WHO Disability Adjusted Life Years (DALY)[15] data. Those diseases for which pharmaceutical interventions were irrelevant (such as violent death, trauma and snakebites) are excluded. In the 2016 Index, the disease scope will consist of a combination of the following:
- The top 10 communicable diseases based on DALYs from the WHO Global Health Observatory 2012 DALY Estimates[16]
- The top 12 non-communicable diseases based on DALYs from the WHO Global Health Observatory 2012 DALY Estimates[16]
- 17 of the WHO Neglected Tropical Diseases[17]
- 9 maternal and neonatal health conditions identified by the WHO Global Health Observatory.[16] In addition, the Index captures activity on contraceptives.
Product type scope[1]
To reflect the range of available product types for prevention, diagnosis and treatment of diseases, the Index maintains a broad product type scope which draws closely from definitions provided by the G-Finder Report.[18]
Index coverage and use
Since its inception, the Access to Medicine Index has progressed to be a frequently cited and ‘authoritative’ benchmark for pharmaceutical companies with regard to their access to medicine initiatives. In addition to global media outlets reporting on the Access to Medicine Index and its findings, significant coverage includes:
- In July 2008, Bill Gates mentioned the Access to Medicine Index in an interview with Time Magazine as an example of an incentive that works to give businesses credit for what they are already doing to address the challenges of access to medicine in developing countries.[19]
- Paul Hunt (academic), the former UN Special Rapporteur on the right to health, describes the Index as a way to measure the pharmaceutical industry's progress in line with human rights obligations in a 2010 PLOS Medicine report.[20]
- The Index was also cited in a 2010 UBS report as a tool for investors to assess access to medicine specifically and, where necessary, separately from corporate social responsibility (CSR) frameworks.[21]
- Since 2008, the Access to Medicine Index has been repeatedly cited in such scientific journals as the British Medical Journal,[22][23] The Lancet[24][25] and The Pharmaceutical Journal.[26]
- Data from the 2014 Index was used in a study of access to hepatitis C medicines in the Bulletin of the World Health Organization.[27]
- The Index was also highlighted as a key source for a 2014 Deutsche Bank report on pharmaceutical industry investment in malaria and neglected tropical diseases.[28]
Criticism
The results of the Access to Medicine Index are largely based on company data provided by the pharmaceutical companies themselves. Self-reported data does carry with it an inherent risk, but the Access to Medicine Index also uses dependable external sources to verify data provided by the companies wherever possible. Additionally, it is in companies’ best interest to be as forthcoming as possible, as they are a) rated by the Index on their degree of transparency and b) rated on their performance every 2 years, so that failures to meet their commitments and/or inconsistencies over time are likely to be uncovered. Besides, as drug access is only one dimension of the Corporate Social Responsibility (CSR) within the pharmaceutical industry, it would not be reasonable to evaluate the CSR practices of pharmaceutical companies only using this index.
References
- 1 2 3 4 5 6 7 8 9 Access to Medicine Foundation. "The 2016 Access to Medicine Index: Methodology 2015" (PDF). Access to Medicine Foundation. Retrieved 29 October 2015.
- ↑ Access to Medicine Foundation. "What is the Index?". Retrieved 29 October 2015.
- ↑ World Health Organization. "Medicines in Health Systems" (PDF). WHO. Retrieved 27 October 2015.
- ↑ UK Department for International Development. "The Access to Medicine Index: Encouraging global access to health care". DFID News. DFID. Retrieved 11 March 2013.
- ↑ Access to Medicine Foundation. "2016 Access to Medicine Index" (PDF). Retrieved 14 November 2016.
- 1 2 Levy, Gideon. "Patents or Patients". AVRO. Retrieved 11 March 2013.
- ↑ "Ranking & Scoring Process". Access to Medicine Foundation. Retrieved 13 June 2013.
- ↑ Access to Medicine Foundation. "Methodology Report 2013 for the 2014 Access to Medicine Index" (PDF). Retrieved 29 October 2015.
- ↑ Access to Medicine Foundation. "2012 Methodology Report - Stakeholder Review" (PDF). Retrieved 29 October 2015.
- ↑ Access to Medicine Foundation. "2010 Methodology Report - Stakeholder Review" (PDF). Retrieved 29 October 2015.
- ↑ Access to Medicine Foundation. "2008 Methodology Report - Stakeholder Review" (PDF). Retrieved 29 October 2015.
- ↑ "How we classify countries". World Bank. Retrieved 11 March 2013.
- ↑ "Least Developed Countries: UN Classification". The World Bank. Retrieved 11 March 2013.
- ↑ UN Capital Development Fund. "Least Developed Countries". Retrieved 27 October 2015.
- ↑ "Health statistics and health information systems: DALY". World Health Organization. Retrieved 11 March 2013.
- 1 2 3 World Health Organization. "WHO methods and data sources for global burden of diseases estimates 2000-2011" (PDF). WHO. Retrieved 27 October 2015.
- ↑ "The 17 neglected tropical diseases". World Health Organization. Retrieved 18 November 2014.
- ↑ "G-Finder 2014. Neglected Disease Research and Development: Emerging Trends". Policy Cures. Retrieved 27 October 2015.
- ↑ Gates & Kiviat, Bill, Barbara (31 July 2008). "Making Capitalism More Creative". Time Magazine. Retrieved 11 March 2013.
- ↑ Hunt & Khosla, Paul, Rajat. "Are Drug Companies Living Up to Their Human Rights Responsibilities? The Perspective of the Former United Nations Special Rapporteur (2002-2008)". PLOS Medicine. Retrieved 11 March 2013.
- ↑ "Global Pharma: Doing well by doing good?" (PDF). UBS Investment Research. Retrieved 18 June 2013.
- ↑ Yudkin, John S. "Post-marketing observational trials and catastrophic health expenditure". British Medical Journal. Retrieved 11 March 2013.
- ↑ Gulland, Anne. "Top drug companies are making more accessible but are also guilty of corruption, report says". British Medical Journal. Retrieved 28 October 2015.
- ↑ Ali & Narayan, Mohammed K., KM Venkat. "The New Access to Medicine Index". The Lancet. Retrieved 11 March 2013.
- ↑ Newsdesk (August 2010). "Bridging the gap in access to medicines" (PDF). The Lancet. 10: 514–515. doi:10.1016/s1473-3099(10)70150-x. Retrieved 11 March 2013.
- ↑ Connelly, Dawn. "Targeting disease in the developing world". The Pharmaceutical Journal. Retrieved 28 October 2015.
- ↑ Edwards; et al. "Access to hepatitis C medicines" (PDF). Bulletin of the World Health Organization. Retrieved 27 October 2015.
- ↑ Deutsch Bank. "F.I.T.T. for investors: Tropical diseases; social responsibility, neglected market" (PDF). Retrieved 28 October 2015.
External links
- The 2016 Access to Medicine Index - Methodology 2015
- The Access to Medicine Index 2014
- Methodology Report 2013 for the 2014 Access to Medicine Index
- 2012 Access to Medicine Index
- 2012 Methodology Report- Stakeholder Review
- 2010 Access to Medicine Index
- 2010 Methodology & Stakeholder Review
- 2008 Access to Medicine Index
- 2008 Industry & Stakeholder Review