Carpal tunnel surgery
Carpal tunnel surgery, also called carpal tunnel release (CTR) and carpal tunnel decompression surgery, is a surgery in which the transverse carpal ligament is divided. It is a treatment for carpal tunnel syndrome and recommended when there is static (constant, not just intermittent) numbness, muscle weakness, or atrophy, and when night-splinting no longer controls intermittent symptoms of pain in the carpal tunnel.[1] In general, milder cases can be controlled for months to years, but severe cases are unrelenting symptomatically and are likely to result in surgical treatment.[2]
Medical uses
The procedure is used as a treatment to carpal tunnel syndrome and is intended to provide relief.
Technique

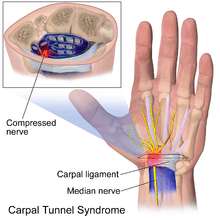
The goal of any carpal tunnel release surgery is to divide the transverse carpal ligament and the distal aspect of the volar ante brachial fascia, thereby decompressing the median nerve and providing relief.[3] The transverse carpal ligament is a wide ligament that runs across the hand, from the scaphoid bone to the hamate bone and pisiform. It forms the roof of the carpal tunnel, and when the surgeon cuts across it (i.e., in a line with the ring finger) it no longer presses down on the nerve inside, relieving the pressure.[4]
The two major types of surgery are open carpal tunnel release and endoscopic carpal tunnel release. Most surgeons historically have performed the open procedure, widely considered to be the gold standard. However, since the 1990s, a growing number of surgeons now offer endoscopic carpal tunnel release.[5] Existing research does not show significant differences in outcomes of one kind of surgery versus the other, so patients can choose a surgeon they like and the surgeon also will practice the technique they like.[6]
Historically, carpal tunnel release was performed under general anaesthesia with a tourniquet, however the worldwide trend is now for 'wide awake hand surgery': with no tourniquet, no general or regional anaesthesia and no sedation; which also enables carpal tunnel release to be performed under local anaesthesia as a one stop procedure.[7]
After carpal tunnel surgery, the long term use of a splint on the wrist should not be used for relief.[8] Splints do not improve grip strength, lateral pinch strength, or bowstringing.[8] While splints may protect people working with their hands, using a splint does not change complication rates or patient satisfaction.[8] Using splints can cause problems including adhesion and lack of flexibility.[8]
Carpal tunnel surgery is usually performed by a hand surgeon, orthopaedic surgeon, or plastic surgeon. Some neurosurgeons and general surgeons also perform the procedure.
Open surgery

Open surgery involves an incision on the palm about an inch or two in length. Through this incision, the skin and subcutaneous tissue is divided, followed by the palmar fascia, and ultimately the transverse carpal ligament.[9][10]
The open release technique has been compared to other treatments.[11]
Endoscopic carpal tunnel release
Endoscopic techniques for carpal tunnel release involve one or two smaller incisions (less than half inch each) through which instrumentation is introduced including a synovial elevator, probes, knives, and an endoscope used to visualize the underside of the transverse carpal ligament.[12] The endoscopic methods do not divide the subcutaneous tissues or the palmar fascia to the same degree as the open method does.[13] Many studies have been done to determine whether perceived benefits of a limited endoscopic or arthroscopic release are significant.
Many surgeons have embraced limited incision methods. It is considered to be the procedure of choice for many of these surgeons with respect to idiopathic carpal tunnel syndrome. Supporting this are the results of some of the previously mentioned series that cite no difference in the rate of complications for either method of surgery. Thus, there has been broad support for either surgical procedure using a variety of devices or incisions.
Thread carpal tunnel release

The thread carpal tunnel release (TCTR) is a minimally invasive procedure for transecting the transverse carpal ligament (TCL) by sawing a piece of thread looped percutaneously under the guidance of ultrasound. The TCTR is performed under local anesthesia in a clinic based procedure room, and results in only one needle entry point at the palm and one needle exit point in the wrist. The technique ensures that the division happens only inside the loop of the thread around the TCL without injuring adjacent tissures. The features of the procedure incluses the potentials of reduced risk of iatrogenic injury, reduced surgical cost, and reduced patient recovery time.[14][15][16]
Risks and complications
Carpal tunnel syndrome cannot be cured, but surgery to alleviate symptoms can be successful. The success rate of surgery to relieve symptoms depends on the definition of “success” and the metrics applied. For example, with respect to alleviation of symptoms, up to 90% success is reported. Yet with respect to patient satisfaction, approximately 50% is reported. The rate at which patients return to their former employer also is less than 90%. Yet approximately 25% of those patients are re-tasked to another duty in order to minimize further stress on their hands.[17][18][19] In general, endoscopic techniques are as effective as traditional open carpal surgeries,[20][21] though the faster recovery time typically noted in endoscopic procedures is felt by some to possibly be offset by higher complication rates.[22][23] Success is greatest in patients with the most typical symptoms. The most common cause of failure is incorrect diagnosis, and it should be noted that this surgery will only mitigate carpal tunnel syndrome, and will not relieve symptoms with alternative causes. Recurrence is rare, and apparent recurrence usually results from a misdiagnosis of another problem. Complications can occur, but serious ones are infrequent to rare.
Recovery
In these surgeries, the flexor retinaculum is either simply severed or lengthened. When surgery is done to divide the flexor retinaculum (which is by far the more common procedure), scar tissue will eventually fill the gap left by surgery. The intent is that this will lengthen the flexor retinaculum enough to accommodate inflamed or damaged tendons and reduce the effects of compression on the median nerve
Research
Balloon carpal tunnelplasty is an experimental technique that uses a minimally invasive balloon catheter director to access the carpal tunnel. As with a traditional tissue elevator/expander, balloon carpal tunnelplasty elevates the carpal ligament, increasing the space in the carpal tunnel. As an experiment it has been described but there are no peer reviewed series available in the current hand surgical literature that review or comment upon the procedure. The technique is performed through a one-centimeter incision at the distal wrist crease. It is monitored and expansion is confirmed by direct or endoscopic visualization. The technique's secondary goals are to avoid to incision in the palm of the hand, to avoid cutting of the transverse carpal ligament, and to maintain the biomechanics of the hand.[24]
References
- ↑ Hui, A.C.F.; Wong, S.M.; Tang, A.; Mok, V.; Hung, L.K.; Wong, K.S. (2004). "Long-term outcome of carpal tunnel syndrome after conservative treatment". International Journal of Clinical Practice. 58 (4): 337–9. doi:10.1111/j.1368-5031.2004.00028.x. PMID 15161116.
- ↑ Kouyoumdjian, JA; Morita, MP; Molina, AF; Zanetta, DM; Sato, AK; Rocha, CE; Fasanella, CC (2003). "Long-term outcomes of symptomatic electrodiagnosed carpal tunnel syndrome". Arquivos de neuro-psiquiatria. 61 (2A): 194–8. doi:10.1590/S0004-282X2003000200007. PMID 12806496.
- ↑ "Carpal Tunnel Syndrome - Your Orthopaedic Connection - AAOS". Orthoinfo.aaos.org. 2009-12-01. Retrieved 2011-10-05.
- ↑ http://www.handuniversity.com/topics.asp?Topic_ID=16 A patient's guide to endoscopic carpal tunnel release
- ↑ Rodner, Craig M.; Katarincic, Julia. (2006)"Open Carpal Tunnel Release". Techniques in Orthopaedics ®21(1):3–11 © 2006 Lippincott Williams & Wilkins, Inc.<http://nemsi.uchc.edu/clinical_services/orthopaedic/handwrist/pdfs/article_carpaltunnel.pdf>
- ↑ Scholten, Rob JPM; Mink van der Molen, Aebele; Uitdehaag, Bernard MJ; Bouter, Lex M; de Vet, Henrica CW; Scholten, Rob JPM (2007). "Surgical treatment options for carpal tunnel syndrome". Reviews. doi:10.1002/14651858.CD003905.pub3.
- ↑ Bismil, M.; Bismil, Q.; Harding, D.; Harris, P.; Lamyman, E.; Sansby, L. (2012). "Transition to total one-stop wide-awake hand surgery service-audit: a retrospective review". JRSM Short Reports. 3 (4): 23–23. doi:10.1258/shorts.2012.012019.
- 1 2 3 4 American Academy of Orthopaedic Surgeons (February 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American Academy of Orthopaedic Surgeons, retrieved 19 May 2013, which cites
- Keith, MW; Masear, V; Chung, KC; Amadio, PC; Andary, M; Barth, RW; Maupin, K; Graham, B; Watters WC, 3rd; Turkelson, CM; Haralson RH, 3rd; Wies, JL; McGowan, R; American Academy of Orthopaedic Surgeons (Jan 2010). "American Academy of Orthopaedic Surgeons clinical practice guideline on the treatment of carpal tunnel syndrome.". The Journal of bone and joint surgery. American volume. 92 (1): 218–9. doi:10.2106/JBJS.I.00642. PMID 20048116.
- ↑ Ariyan, S; Watson, HK (1977). "The palmar approach for the visualization and release of the carpal tunnel. An analysis of 429 cases". Plast Reconstr Surg. 60 (4): 539–547. doi:10.1097/00006534-197710000-00007. PMID 909963.
- ↑ Nigst H (1992) The carpal tunnel syndrome. Operative technique for surgical decompression. Orthop and Traumat 1, 122–129
- ↑ Vasiliadis, Haris S; Sakellaridou, Maria Eleni; Shrier, Ian; Salanti, Georgia; Scholten, Rob JPM; Vasiliadis, Haris S (2014). "Open release for carpal tunnel syndrome". Protocols. doi:10.1002/14651858.CD011041.
- ↑ https://www.youtube.com/watch?v=M4hTY1vyrxg[]
- ↑ Agee, JM; et al. "Endoscopic release of the carpal tunnel: A randomized prospective multicenter study". The Journal of Hand Surgery. 17 (6): 987–995. doi:10.1016/S0363-5023(09)91044-9.
- ↑ Guo, Danqing; Tang, Yu; Ji, Yizheng; Sun, Tiansheng; Guo, Joseph; Guo, Danzhu (2014-06-06). "A non-scalpel technique for minimally invasive surgery: percutaneously looped thread transection of the transverse carpal ligament". HAND. 10 (1): 40–48. doi:10.1007/s11552-014-9656-4. ISSN 1558-9447. PMC 4349829
 . PMID 25767420.
. PMID 25767420. - ↑ Guo, Danqing; Guo, Danzhu; Guo, Joseph; Malone, Daniel; Wei, Nathan; McCool, Logan (2016-08-20). "A Cadaveric Study for the Improvement of Thread Carpal Tunnel Release". Journal of Hand Surgery (2016). doi:10.1016/j.jhsa.2016.07.098.
- ↑ Guo, Danqing; Guo, Danzhu; Guo, Joseph; Schmidt, Steven; Lytie, Rachel (2016-09-12). "A Clinical Study of the Modified Thread Carpal Tunnel Release (TCTR)". HAND (2016). doi:10.1177/1558944716668831.
- ↑ Schmelzer, Rodney E.; Rocca, Gregory J. Della; Caplin, David A. (2006). "Endoscopic Carpal Tunnel Release: A Review of 753 Cases in 486 Patients". Plastic and Reconstructive Surgery. 117 (1): 177–85. doi:10.1097/01.prs.0000194910.30455.16. PMID 16404264.
- ↑ Quaglietta, Paolo; Corriero, G. (2005). "Advanced Peripheral Nerve Surgery and Minimal Invasive Spinal Surgery". Acta Neurochirurgica Supplementum. Acta Neurochirurgica. 97: 41–5. doi:10.1007/3-211-27458-8_10. ISBN 3-211-23368-7.
|chapter=ignored (help) - ↑ Park, S.-H.; Cho, B. H.; Ryu, K. S.; Cho, B. M.; Oh, S. M.; Park, D. S. (2004). "Surgical Outcome of Endoscopic Carpal Tunnel Release in 100 Patients with Carpal Tunnel Syndrome". Minimally Invasive Neurosurgery. 47 (5): 261–5. doi:10.1055/s-2004-830075. PMID 15578337.
- ↑ Scholten, R; Bouter, LM; Gerritsen, A; Uitdehaag, BM; De Vet, HCW; Van Geldere, D; Scholten, Rob (2004). Scholten, Rob, ed. "The Cochrane Database of Systematic Reviews". Cochrane Database of Systematic Reviews. doi:10.1002/14651858.CD003905.pub2.
|chapter=ignored (help) - ↑ McNally, S. A.; Hales, PF (2003). "Results of 1245 endoscopic carpal tunnel decompressions". Hand Surgery. 8 (1): 111–6. doi:10.1142/S0218810403001480. PMID 12923945.
- ↑ Thoma, Achilleas; Veltri, Karen; Haines, Ted; Duku, Eric (2004). "A Meta-Analysis of Randomized Controlled Trials Comparing Endoscopic and Open Carpal Tunnel Decompression". Plastic and Reconstructive Surgery: 1137–46. doi:10.1097/01.PRS.0000135850.37523.D0.
- ↑ Chow, J; Hantes, M (2002). "Endoscopic carpal tunnel release: Thirteen years' experience with the chow technique". The Journal of Hand Surgery. 27 (6): 1011–8. doi:10.1053/jhsu.2002.35884. PMID 12457351.
- ↑ Berger, L. "Balloon Carpal Tunnelplasty, First Comparative Clinical Study" The University of Pittsburgh Journal Vol 17, pg 80; 2006