Corrective lens


A corrective lens is a lens worn in front of the eye, mainly used to treat myopia, hyperopia, astigmatism, and presbyopia. Glasses or "spectacles" are worn on the face a short distance in front of the eye. Contact lenses are worn directly on the surface of the eye. Intraocular lenses are surgically implanted most commonly after cataract removal, but recently for purely refractive purposes. Myopia (near-sightedness) requires a divergent lens, whereas hyperopia (far-sightedness) requires a convergent lens.
Prescription of corrective lenses
Corrective lenses are typically prescribed by an ophthalmologist or an optometrist. The prescription consists of all the specifications necessary to make the lens. Prescriptions typically include the power specifications of each lens (for each eye). Strengths are generally prescribed in quarter-diopter steps (0.25 D) because most people cannot generally distinguish between smaller increments (e.g., eighth-diopter steps / 0.125 D).
Components of a sphero-cylindrical correction
Sphere component
Every corrective lens prescription includes a spherical correction in diopters. Convergent powers are positive (e.g., +4.00 D) and condense light to correct for farsightedness (hyperopia) or allow the patient to read more comfortably (see presbyopia and binocular vision disorders). Divergent powers are negative (e.g., −3.75 D) and spread out light to correct for nearsightedness (myopia). If neither convergence nor divergence is required in the prescription, "plano" is used to denote a refractive power of zero.
The term "sphere" comes from the concept that the basic geometry of a corrective lens is a series of curved surfaces that are sections of spheres. These surfaces can be modified as needed to generate more complex corrections by using more complex geometry. The "cylinder" and "axis" components specify how a particular lens is different from a lens composed of purely spherical surfaces.
Cylinder component
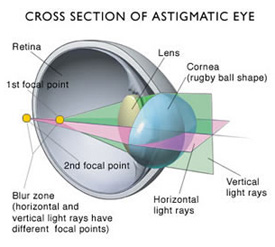
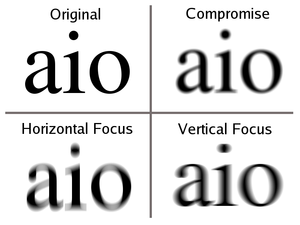
Patients with astigmatism need a toric lens to see clearly. The geometry of a toric lens focuses light differently in different meridians. For example, a toric lens, when rotated correctly, could focus a horizontal line to a series of points at one focal distance while focusing a vertical line to a separate focal plane. This photo helps to illustrate this concept.
{kind=link}
The power of a toric lens can be specified by describing how the cylinder (the meridian that is most different from the spherical power) differs from the spherical power. Power evenly transitions between the two powers as you move from the meridian with the most convergence to the meridian with the least convergence or most divergence. For regular toric lenses, these powers are perpendicular to each other and their location relative to vertical and horizontal are specified by the axis component.
There are two different conventions for indicating the amount of cylinder: "plus cylinder notation" and "minus cylinder notation". In the former, the cylinder power is a number of diopters more convergent than the sphere power. That means the spherical power describes the most divergent meridian and the cylindrical component describes the most convergent. In the latter, the cylinder power is a number of diopters more divergent than the sphere component. Thus the sphere power describes the most convergent meridian and the cylinder component describes the most divergent. Europe typically follows the plus cylinder convention while the US typically follows the minus cylinder convention. Minus cylinder notation is also more common in Asia, although either style may be encountered there. There is no difference in these forms of notation and it is easy to convert between them: simply add the sphere and cylinder numbers together to produce the converted sphere—then change the sign of the cylinder number. For example, a lens with a vertical power of -3.75 and a horizontal power of -2.25 could be specified as either -2.25, -1.50 or -3.75, +1.50.
Axis component

The axis defines the location of the sphere and cylinder powers. The name "axis" comes from the concept of generating a cylinder by rotating a one line around an axis. The curve of that cylinder is 90° from that axis of rotation. When dealing with toric lenses, the axis defines the orientation of the steepest and flattest curvatures relative to horizontal and vertcal. The "3 o'clock" position is defined as zero, and the 90th meridian is a vertical line. A horizontal line passes through both zero and the 180th meridians. By convention, a horizontal axis is recorded as 180.
In a typical toric lens, the flattest and steepest curvatures are separated by 90°. As a result, the axis of the cylinder is also the meridian containing the sphere power. The cylinder power, as defined above is the power that is most different from the sphere power. Because they are defined relative to each other, it is important to know if the lens is being described in minus cylinder notation, where the sphere power is the most convergent / least divergent power. When using plus cylinder notation, the opposite is true.
If the lens is spherical (there is no cylinder component) then there is no need for an axis. A prescription like this is written with D.S. (diopters sphere) after the spherical power (e.g., −3.00 D.S.).
Summary
- correction power is measured in diopters
- by convention, an axis of 90° is vertical, 0° or 180° are horizontal
- if the cylinder power is positive, the lens is most convergent 90° from the axis
- if the cylinder power is negative, the lens is most divergent 90° from the axis
- if the cylinder power is zero (D.S.), the lens is spherical and has the same power in every meridian
Sample prescription
A prescription of −1.00 +0.25 x 180 describes a lens that has a horizontal power of −1.00 D and a vertical power of −0.75.
Other considerations
Single vision lenses correct for only distance or near vision. Patients with presbyopia or other disorders of accommodation often benefit from corrections for both distance and near vision (see Lens Types below). Infrequently, prism and base curve values may also be specified to correct for binocular vision disorders.
Over the counter correction
Over the counter glasses are available without a prescription. They are used to lessen the focusing burden of near work and, in some cases, mild farsightedness (hyperopia). While these "magnifiers" or "ready readers" as they are often called do indeed make the image of the viewed object bigger, the main advantage comes from the power of the lens. Over the counter readers are spherical corrective lenses of varying powers (commonly +1.00 D to +4.00 D). These lenses bend light coming from near objects making it more similar to light coming from distant objects.
These glasses are not as tailored to the specific needs of the patient. A difference in refractive error between the eyes or presence of astigmatism will not be accounted for. The use of improper corrective lenses may not help or could even exacerbate binocular vision disorders. Over the counter glasses do not usually correct for distance vision. Eyecare professionals (optometrists and ophthalmologists) are trained to determine the specific corrective lenses that will provide the clearest, most comfortable and most efficient vision, avoiding double vision and maximizing binocularity. They can test to see if over the counter corrective lenses are appropriate.
Lens types
Single vision

Single vision lenses correct for only one distance. If they correct for far distance, the person must accommodate to see clearly up close. If the person cannot accommodate, they may need a separate pair of single vision glasses for near distances, or else use a multifocal lens (see below).
Bifocal
With bifocals, the upper part of the lens is generally used for distance vision, while the lower segment is used for near vision. The area of the lens that caters to near vision is called the add segment. There are many different shapes, sizes, and positions for the add segment that are selected for functional differences as well as the visual demands of the patient. Bifocals allow people with presbyopia to see clearly at distance and near without having to remove the glasses, which would be required with single vision correction.
Usually, a segment line separates the two segments. Typically a person with myopia would have one section of a prescription lens that has a certain diverging power while another section of the lens would have a lower diverging power for close-up work. Similarly a person with hyperopia would have one section of the lens with a certain converging power and another section with a greater power for close-up work.
Trifocal
Trifocal lenses are similar to bifocals, except that the two focal areas are separated by a third area (with intermediate focus correction) in the middle. This segment corrects the wearer's vision for intermediate distances roughly at arms' length, e.g. computer distance. This lens type has two segment lines, dividing the three different correcting segments.
Progressive
Progressive addition or varifocal lenses provide a smooth transition from distance correction to near correction, eliminating segment lines and allowing clear vision at all distances, including intermediate (roughly arms' length).[1] The lack of any abrupt change in power and the uniform appearance of the lens gives rise to the name "no-line bifocal".
Adjustable focus
Adjustable or variable focus dynamically adjusts focal length, typically allowing clear vision at any distance. It is especially useful for treating the loss of accommodation common in presbyopia.
Plano
Some people with good natural eyesight like to wear eyeglasses as a style accessory, or want to change the appearance of their eyes using novelty contact lenses. For these people, no power or acuity correction is required. Some may need a prescription in one lens in their spectacles, but not in the other. In this case the lens is simply a placeholder that does nothing, with equal parallel curved surfaces. This is referred to as a plano lens.
Over-the-counter reading glasses
Ready-made single-vision reading glasses go by many names, including over-the-counter glasses, ready readers, cheaters, magnifiers, non-prescription readers, or generic readers. They offer clearer vision to people with presbyopia and hyperopia. They are typically sold in retail locations such as pharmacies and grocery stores, but are also available in book stores and clothing retailers. They are available in common reading prescriptions in strengths ranging from +0.75 to +3.50 diopters.
Such glasses do not take into account the possible need for any astigmatism correction, which will influence both the near and the distance prescription. The need for a cylindrical component in the otherwise spherical lens surfaces, correctly aligned in angle, is used to correct for astigmatism, and any lack of such correction is a major cause of tiredness and headaches in people doing prolonged close work or reading. If the wearer has little to no need for the correction of astigmatism, off-the-shelf glasses may work quite well for seeing better during near vision tasks. But if the person has a need for distance correction, it is less likely that they will be perfectly effective.
Reading glasses come in two main styles: full frames, in which the entire lens is made in the reading prescription, and half-eyes, style glasses that sit lower down on the nose.[2] Full frame readers must be removed to see distance clearly, while the distance can be clearly viewed over the top of half-eye readers.
Although such glasses are generally considered safe, an individual prescription, as determined by an ophthalmologist or optometrist and made by a qualified optician, usually results in better visual correction and fewer headaches and visual discomfort. This is due to the optical centres of the lenses in non prescription readers not being correctly aligned with the wearers Pupillary Distance (the distance between pupils). This can cause headaches, discomfort and in some cases eye muscle strain due to prismatic effects.
However there is no recorded study that shows any long-term damage can occur due to using these standard off-the-shelf glasses; the only valid argument being that serious problems of a medical kind may be missed if a professional examination is not conducted by a trained diagnostic optometrist or ophthalmologist.
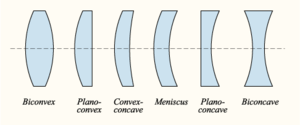
Lens optical profile
Although corrective lenses can be produced in many different profiles, the most common is ophthalmic or convex-concave. In an ophthalmic lens, both the front and back surface have a positive radius, resulting in a positive / convergent front surface and a negative / divergent back surface. The difference in curvature between the front and rear surface leads to the corrective power of the lens. In hyperopia a convergent lens is needed, therefore the convergent front surface overpowers the divergent back surface. For myopia the opposite is true: the divergent back surface is greater in magnitude than the convergent front surface. To correct for presbyopia, the lens, or section of the lens, must be more convergent or less divergent than the person's distance lens.
The base curve (usually determined from the profile of the front surface of an ophthalmic lens) can be changed to result in the best optic and cosmetic characteristics across the entire surface of the lens. Optometrists may choose to specify a particular base curve when prescribing a corrective lens for either of these reasons. A multitude of mathematical formulas and professional clinical experience has allowed optometrists and lens designers to determine standard base curves that are ideal for most people. As a result, the front surface curve is more standardized and the characteristics that generate a person's unique prescription are typically derived from the geometry of the back surface of the lens.
Bifocals and trifocals
Bifocals and trifocals result in a more complex lens profile, compounding multiple surfaces. The main lens is composed of a typical ophthalmic lens. Thus the base curve defines the front surface of the main part of the lens while the back surface geometry is changed to achieve the desired distance power. The "bifocal" is a third spherical segment, called an add segment, found on the front surface of the lens. Steeper and more convergent than the base curve, the add segment combines with the back surface to deliver the person's near correction. Early manufacturing techniques fused a separate lens to the front surface, but modern processes cut all the geometry into a single piece of lens material. There are many locations, profiles, and sizes of add segments, typically referred to as segment type. Some "seg type" examples include Flat top, Kryptok, Orthogon, Tillyer Executive, and Ultex A. Trifocals contain two add segments to achieve a lens that corrects the person's vision for three distinct distances.
The optical center of the add segment may be placed on the lens surface or may hang off into empty space near the lens surface. Although the surface profile of a bifocal segment is spherical, it is often trimmed to have straight edges so that it is contained within a small region of the overall lens surface.
Progressive lens
The progressive addition lens (PAL, also commonly called a no-line or varifocal lens) eliminates the line in bi/tri-focals and is very complex in its profile. PALs are a continuously variable parametric surface that begins using one spherical surface base curve and ends at another, with the radius of curvature continuously varying as the transition is made from one surface to the other. This shift in curvature results in different powers being delivered from different locations on the lens.
Lens distance from eye
"Vertex distance" is the space between the front of the eye and the back surface of the lens. In glasses with powers greater than four diopters, the vertex distance can affect the effective power of the glasses.
The overall size of the lens is controlled by how far the lens is positioned away from the eyes. A closer distance allows for a smaller lens, but there is a limit on how close eyeglass lenses in a frame can be to the eye, imposed by the eyelashes and eyelid.
Contact lenses placed directly on the cornea are physically larger than the pupillary region, and have a ring of extra unused material around the outer perimeter that simply helps to center the lens on the cornea.
Eyeglass lenses need to be larger the further away they are from the eye. Very large lenses in a double-bridge frame do not necessarily provide greater peripheral vision, due to the nose rest holding the lenses slightly further away from the eyes than with smaller lens frames.
Refractive index
In the UK and the US, the refractive index is generally specified with respect to the yellow He-d Fraunhofer line, commonly abbreviated as nd. Lens materials are classified by their refractive index, as follows:
- Normal index – 1.48 ≤ nd < 1.54
- Mid-index – 1.54 ≤ nd < 1.60
- High-index – 1.60 ≤ nd < 1.74
- Very high index – 1.76 ≤ nd
This is a general classification. Indexes of nd values that are ≥ 1.60 can be, often for marketing purposes, referred to as high-index. Likewise, Trivex and other borderline normal/mid-index materials, may be referred to as mid-index.
Advantages of higher indices
- Thinner, sometimes lighter lenses (See below).
- Improved UV protection over CR-39 and glass lenses.
Disadvantages of increased indices
- Lower Abbe number meaning, amongst other things, increased chromatic aberration.
- Poorer light transmission and increased backside and inner-surface reflections (see Fresnel reflection equation) increasing importance of anti-reflective coating.
- Manufacturing defects have more impact on optical quality..
- Theoretically, off-axis optical quality degrades (oblique astigmatic error). In practice this degradation should not be perceptible – current frame styles are much smaller than they would have to be for these aberrations to be noticeable to the patient, the aberration occurring some distance away from the optical centre of the lens (off-axis).
Optical quality
Abbe number
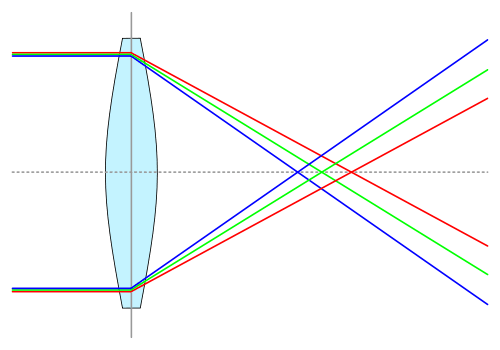


Of all of the properties of a particular lens material, the one that most closely relates to its optical performance is its dispersion, which is specified by the Abbe number. Lower Abbe numbers result in the presence of chromatic aberration (i.e., color fringes above/below or to the left/right of a high contrast object), especially in larger lens sizes and stronger prescriptions (±4D or greater). Generally, lower Abbe numbers are a property of mid and higher index lenses that cannot be avoided, regardless of the material used. The Abbe number for a material at a particular refractive index formulation is usually specified as its Abbe value.
In practice, a change from 30 to 32 Abbe will not have a practically noticeable benefit, but a change from 30 to 47 could be beneficial for users with strong prescriptions that move their eyes and look "off-axis" of optical center of the lens. Note that some users do not sense color fringing directly but will just describe "off-axis blurriness". Abbe values even as high as that of (Vd≤45) produce chromatic aberrations which can be perceptible to a user in lenses larger than 40 mm in diameter and especially in strengths that are in excess of ±4D. At ±8D even glass (Vd≤58) produces chromatic aberration that can be noticed by a user. Chromatic aberration is independent of the lens being of spherical, aspheric, or atoric design.
The eye's Abbe number is independent of the importance of the corrective lens's Abbe, since the human eye:
- Moves to keep the visual axis close to its achromatic axis, which is completely free of dispersion (i.e., to see the dispersion one would have to concentrate on points in the periphery of vision, where visual clarity is quite poor)
- Is very insensitive, especially to color, in the periphery (i.e., at retinal points distant from the achromatic axis and thus not falling on the fovea, where the cone cells responsible for color vision are concentrated. See: Anatomy and Physiology of the Retina.)
In contrast, the eye moves to look through various parts of a corrective lens as it shifts its gaze, some of which can be as much as several centimeters off of the optical center. Thus, despite the eye's dispersive properties, the corrective lens's dispersion cannot be dismissed. People who are sensitive to the effects of chromatic aberrations, or who have stronger prescriptions, or who often look off the lens’s optical center, or who prefer larger corrective lens sizes may be impacted by chromatic aberration. To minimize chromatic aberration:
- Try to use the smallest vertical lens size that is comfortable. Generally, chromatic aberrations are more noticeable as the pupil moves vertically below the optical center of the lens (e.g., reading or looking at the ground while standing or walking). Keep in mind that a smaller vertical lens size will result in a greater amount of vertical head movement, especially while performing activities that involve short and intermediate distance viewing, which could lead to an increase in neck strain, especially in occupations involving a large vertical field of view.
- Restrict the choice of lens material to the highest Abbe value at acceptable thickness. The oldest most basic commonly used lens materials also happen to have the best optical characteristics at the expense of corrective lens thickness (i.e., cosmetics). Newer materials have focused on improved cosmetics and increased impact safety, at the expense of optical quality. Lenses sold in the USA must pass the Food and Drug Administration ball-drop impact test, and depending on needed index these seem to currently have"‘best in class" Abbe vs Index (Nd): Glass (2x weight of plastics) or CR-39 (2 mm vs. 1.5 mm thickness typical on newer materials) 58 @ 1.5, Sola Spectralite ([email protected]), Sola Finalite ([email protected]), and Hoya Eyry (36 @ 1.7). For impact resistance safety glass is offered at a variety of indexes at high Abbe number, but is still 2x the weight of plastics. Polycarbonate (Vd=30-32) is very dispersive, but has excellent shatter resistance. Trivex (Vd=43 @ 1.53), is also heavily marketed as an impact resistant alternative to Polycarbonate, for individuals who don’t need polycarbonate’s index. Trivex is also one of the lightest materials available.
- Use contact lenses in place of eyeglasses. A contact lens rests directly on the surface of the cornea and moves in sync with all eye movements. Consequently, the contact lens is always directly aligned on center with the pupil and there is never any off-axis misalignment between the pupil and the optical center of the lens.
Power error (-D corrections for myopia)
Power error is the change in the optical power of a lens as the eye looks through various points on the area of the lens. Generally, it is least present at the optic center and gets progressively worse as one looks towards the edges of the lens. The actual amount of power error is highly dependent on the strength of the prescription as well as whether a best spherical form of lens or an optically optimal aspherical form was used in the manufacture of the lens. Generally, best spherical form lenses attempt to keep the ocular curve between four and seven diopters.
Lens induced oblique astigmatism (+D corrections for presbyopia)
As the eye shifts its gaze from looking through the optical center of the corrective lens, the lens-induced astigmatism value increases. In a spherical lens, especially one with a strong correction whose base curve is not in the best spherical form, such increases can significantly impact the clarity of vision in the periphery.
Minimizing power error and lens induced astigmatism
As corrective power increases, even optimally designed lenses will have distortion that can be noticed by a user. This particularly affects individuals that use the off-axis areas of their lenses for visually demanding tasks. For individuals sensitive to lens errors, the best way to eliminate lens induced aberrations is to use contact lenses. Contacts eliminate all these aberrations since the lens then moves with the eye.
Barring contacts, a good lens designer doesn’t have many parameters which can be traded off to improve vision. Index has little effect on error. Note that, although chromatic aberration is often perceived as "blurry vision" in the lens periphery and gives the impression of power error, this is actually due to color shifting. Chromatic aberration can be improved by using a material with improved ABBE. The best way to combat lens induced power error is to limit the choice of corrective lens to one that is in the best spherical form. A lens designer determines the best-form spherical curve using the Oswalt curve on the Tscherning ellipse. This design gives the best achievable optical quality and least sensitivity to lens fitting. A flatter base-curve is sometimes selected for cosmetic reasons. Aspheric or atoric design can reduce errors induced by using a suboptimal flatter base-curve. They cannot surpass the optical quality of a spherical best-form lens, but can reduce the error induced by using a flatter than optimal base curve. The improvement due to flattening is most evident for strong farsighted lenses. High myopes (-6D) may see a slight cosmetic benefit with larger lenses. Mild prescriptions will have no perceptible benefit (-2D). Even at high prescriptions some high myope prescriptions with small lenses may not see any difference, since some aspheric lenses have a spherically designed center area for improved vision and fit.[3]
In practice, labs tend to produce pre-finished and finished lenses in groups of narrow power ranges to reduce inventory. Lens powers that fall into the range of the prescriptions of each group share a constant base curve. For example, corrections from -4.00D to -4.50D may be grouped and forced to share the same base curve characteristics, but the spherical form is only best for a -4.25D prescription. In this case the error will be imperceptible to the human eye. However, some manufacturers may further cost-reduce inventory and group over a larger range which will result in perceptible error for some users in the range who also use the off-axis area of their lens. Additionally some manufacturers may verge toward a slightly flatter curve. Although if only a slight bias toward plano is introduced it may be negligible cosmetically and optically. These optical degradations due to base-curve grouping also apply to aspherics since their shapes are intentionally flattened and then asphericized to minimize error for the average base curve in the grouping.
Self refraction
Although lenses are normally prescribed by optometrists or ophthalmologists, there is evidence from developing countries that allowing people to select lenses for themselves produces good results in the majority of cases and is less than a tenth of the cost of prescription lenses.[4] In addition, if distributed manufacturing with 3-D printers is used the cost of the glasses drops further.[5] In a study published by Zhang in 2011 of 648 young Chinese people (mean age 14.9 years), differences between subjective refraction (formal testing by an optometrist or ophthalmologist) and self refraction (allowing the children to choose the lenses that suited them best) were very close. With self refraction, 97% of participants were able to achieve a visual acuity of 6/7.5 or better, compared to 99% by subjective refraction.[6] That study goes on to say, "[Patients] with widespread access to high quality refractive services [are] not representative of the populations in which self refraction would likely be used."
Cosmetics and weight
Reducing lens thickness
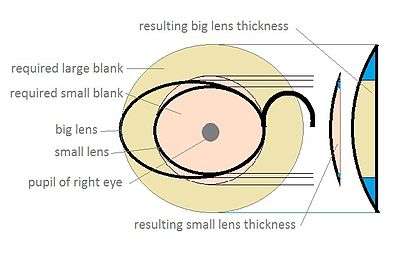
Note that the greatest cosmetic improvement on lens thickness (and weight) is had from choosing a frame which holds physically small lenses. The smallest of the popular adult lens sizes available in retail outlets is about 50 mm (2.0 in) across. There are a few adult sizes of 40 mm (1.6 in), and although they are quite rare, can reduce lens weight to about half of the 50 mm versions. The curves on the front and back of a lens are ideally formed with the specific radius of a sphere. This radius is set by the lens designer based on the prescription and cosmetic consideration. Selecting a smaller lens will mean less of this sphere surface is represented by the lens surface, meaning the lens will have a thinner edge (myopia) or center (hyperopia). A thinner edge reduces light entering into the edge, reducing an additional source of internal reflections.
Extremely thick lenses for myopia can be beveled to reduce flaring out of the very thick edge. Thick myopic lenses are not usually mounted in wire frames, because the thin wire contrasts against the thick lens, to make its thickness much more obvious to others.
Index can improve the lens thinness, but at a point no more improvement will be realized. For example, if an index and lens size is selected with center to edge thickness difference of 1 mm then changing index can only improve thickness by a fraction of this. This is also true with aspheric design lenses.
The lens's minimum thickness can also be varied. The FDA ball drop test (5/8" 0.56 ounce steel ball dropped from 50 inches)[7] effectively sets the minimum thickness of materials. Glass or CR-39 requires 2.0 mm, but some newer materials only require 1.5 mm or even 1.0 mm minimum thickness.
Weight
Material density typically increases as lens thickness is reduced by increasing index. There is also a minimum lens thickness required to support the lens shape. These factors results in a thinner lens which is not lighter than the original. There are lens materials with lower density at higher index which can result in a truly lighter lens. These materials can be found in a material property table. Reducing frame lens size will give the most noticeable improvement in weight for a given material. Ways to reduce the weight and thickness of corrective lenses, in approximate order of importance are these:
- Choose glasses frames with small lenses; that is to say, so that the longest measurement across the lens at any angle is as short as possible. This gives the greatest advantage of all.
- Choose a frame that allows the pupil to occupy the exact middle point of the lens.
- Choose a lens as near round as possible. These are less commonly found than other shapes.
- Choose as high a refractive index for the lens material as cost permits.
It is not always possible to follow the above points, because of the rarity of such frames, and the need for more pleasing appearance. However, these are the main factors to consider if ever it should become necessary and possible to do so.
Facial distortion and social stigma
Eyeglasses for a high-diopter nearsighted or farsighted person cause a visible distortion of his or her face as seen by other people, in the apparent size of the eyes and facial features visible through the eyeglasses.
- For extreme nearsightedness the eyes appear small and sunken into the face, and the sides of the skull can be visible through the lens. This gives the wearer the appearance of having a very large or fat head in contrast with their eyes.
- For extreme farsightedness the eyes appear very large on the face, making the wearer's head seem too small.
Either situation can result in social stigma[8] due to some facial distortions. This can result in low self-esteem of the eyeglass wearer and lead to difficulty in making friends and developing relationships.
People with very high-power corrective lenses can benefit socially from contact lenses because these distortions are minimized and their facial appearance to others is normal. Aspheric/atoric eyeglass design can also reduce minification and magnification of the eye for observers at some angles.
Lens materials
Optical crown glass (B270)
Schott B270 is an optical glass used in precision optics. It is NOT an ophthalmic glass. Schott ophthalmic glass types are S-1 and S-3. The issue here is incorrect numbers for UVA and UVB transmission, as well as other related product type issues.
- Refractive index (nd): 1.52288
- Abbe value (Vd): 58.5
- Density: 2.55 g/cm³ (the heaviest corrective lens material in common use, today)
- UV cutoff: 320 nm
Glass lenses have become less common owing to the danger of shattering and their relatively high weight compared to CR-39 plastic lenses. They still remain in use for specialised circumstances, for example in extremely high prescriptions (currently, glass lenses can be manufactured up to a refractive index of 1.9) and in certain occupations where the hard surface of glass offers more protection from sparks or shards of material. If the highest Abbe value is desired, the only choices for common lens optical material are optical crown glass and CR-39.
Higher-quality optical-grade glass materials exist (e.g. Borosilicate crown glasses such as BK7 (nd=1.51680 / Vd=64.17 / D=2.51 g/cm³), which is commonly used in telescopes and binoculars, and fluorite crown glasses such as Schott N-FK51A (nd=1.48656 / Vd=84.47 / D=3.675 g/cm³), which is 16.2 times the price of a comparable amount of BK7, and are commonly used in high-end camera lenses). However, one would be very hard pressed to find a laboratory that would be willing to acquire or shape custom eyeglass lenses, considering that the order would most likely consist of just two different lenses, out of these materials. Generally, Vd values above 60 are of dubious value, except in combinations of extreme prescriptions, large lens sizes, a high wearer sensitivity to dispersion, and occupations that involve work with high contrast elements (e.g. reading dark print on very bright white paper, construction involving contrast of building elements against a cloudy white sky, a workplace with recessed can or other concentrated small area lighting, etc.).
Plastic
For CR-39:
- Refractive index (nd): 1.498 (standard)
- Abbe value (Vd): 59.3
- Density: 1.31 g/cm³
- UV cutoff: 355 nm
Plastic lenses are currently the most commonly prescribed lens, owing to their relative safety, low cost, ease of production, and high optical quality. The main drawbacks of many types of plastic lenses are the ease by which a lens can be scratched, and the limitations and costs of producing higher-index lenses. CR-39 lenses are an exception in that they have inherent scratch resistance.
Trivex
- Refractive index (nd): 1.532
- Abbe value (Vd): 43–45 (depending on licensing manufacturer)
- Density: 1.1 g/cm³ (the lightest corrective lens material in common use)
- UV cutoff: 380 nm
Trivex was originally developed for the military, as visual armor. PPG Industries took the technology and adapted it for the optical industry. Trivex is a urethane based pre-polymer. PPG named the material Trivex because of its three main performance properties. The three main properties are superior optics, ultra light weight, and extreme strength. Trivex is a relative newcomer that possesses the UV-blocking properties and shatter resistance of polycarbonate while at the same time offering far superior optical quality (i.e., higher Abbe value) and a slightly lower density. Its lower refractive index of 1.532 vs. polycarbonate's 1.586 may result in slightly thicker lenses. Along with polycarbonate and the various high-index plastics, Trivex is a lab favorite for use in rimless frames, owing to the ease with which it can be drilled and its resistance to cracking around the drill holes. One other advantage that Trivex has over polycarbonate is that it can be easily tinted.
Polycarbonate
- Refractive index (nd): 1.586
- Abbe value (Vd): 30
- Density: 1.2 g/cm³
- UV cutoff: 385 nm
Polycarbonate is lighter weight than normal plastic. It blocks UV rays, is shatter resistant and is used in sports glasses and glasses for children and teenagers. Because polycarbonate is soft and will scratch easily, scratch resistant coating is typically applied after shaping and polishing the lens. Standard polycarbonate with an Abbe value of 30 is one of the worst materials optically, if chromatic aberration intolerance is of concern. Along with Trivex and the high-index plastics, polycarbonate is an excellent choice for rimless eyeglasses. Similar to the high-index plastics, polycarbonate has a very low Abbe value, which may be bothersome to individuals sensitive to chromatic aberrations.
High-index plastics (thiourethanes)
- Refractive index (nd): 1.600–1.740
- Abbe value (Vd): 42–32 (higher indexes generally result in lower Abbe values)
- Density: 1.3–1.5 (g/cm³)
- UV cutoff: 380–400 nm
High-index plastics allow for thinner lenses. The lenses may not be lighter, however, due to the increase in density vs. mid- and normal index materials. A disadvantage is that high-index plastic lenses suffer from a much higher level of chromatic aberrations, which can be seen from their lower Abbe value. Aside from thinness of the lens, another advantage of high-index plastics is their strength and shatter resistance, although not as shatter resistant as polycarbonate. This makes them particularly suitable for rimless eyeglasses.
These high-refractive-index plastics are typically thiourethanes, with the sulfur atoms in the polymer being responsible for the high refractive index.[9] The sulfur content can be up to 60 percent by weight for an n=1.74 material.[9]
Ophthalmic material property tables
| Material, Glass | Index (Nd) | ABBE (Vd) | Specific Gravity | UVB/ UVA | Reflected light (%) | Minimum thickness typ/min (mm) | Note |
|---|---|---|---|---|---|---|---|
| Crown Glass | 1.525 | 59 | 2.54 | 79% / 20% | 8.59 | ||
| PhotoGray Extra | 1.523 | 57 | 2.41 | 100% / 97% | 8.59 | ||
| 1.6 Glass | 1.604 | 40 | 2.62 | 100% / 61% | 10.68 | Zeiss Uropal, VisionEase, X-Cel | |
| 1.7 Glass | 1.706 | 30 | 2.93 | 100% / 76% | 13.47 | Zeiss Tital, X-Cel, VisionEase, Phillips | |
| 1.8 Glass | 1.800 | 25 | 3.37 | 100% / 81% | 16.47 | Zeiss Tital, X-Cell, Phillips, VisionEase,Zhong Chuan Optical(China) | |
| 1.9 Glass | 1.893 | 31 | 4.02 | 100% / 76% | 18.85 | Zeiss Lantal, Zhong Chuan Optical(China) not FDA-approved for sale in USA |
Reflected light calculated using Fresnel reflection equation for normal waves against air on two interfaces. This is reflection without an AR coating.
Indices of refraction for a range of materials can be found in the list of refractive indices.
Lens coatings
Anti-reflective

Anti-reflective coatings help to make the eye behind the lens more visible. They also help lessen back reflections of the white of the eye as well as bright objects behind the eyeglasses wearer (e.g. windows, lamps). Such reduction of back reflections increases the apparent contrast of surroundings. At night, anti-reflective coatings help to reduce headlight glare from oncoming cars, street lamps and heavily lit or neon signs.
One problem with anti-reflective coatings is that historically they have been very easy to scratch. Newer coatings, such as Crizal Alizé UV with its 5.0 rating and Hoya's Super HiVision with its 10.9 rating on the COLTS Bayer Abrasion Test (glass averages 12–14), try to address this problem by combining scratch resistance with the anti-reflective coating. They also offer a measure of dirt and smudge resistance, due to their hydrophobic properties (110° water drop contact angle for Super HiVision and 116° for Crizal Alizé UV).
Ultraviolet protection
A UV coating is used to reduce the transmission of light in the ultraviolet spectrum. UV-B radiation increases the likelihood of cataracts, while long-term exposure to UV-A radiation can damage the retina. DNA damage from UV light is cumulative and irreversible. Some materials such as Trivex and Polycarbonate, naturally block most UV light; they have UV-cutoff wavelengths just outside the visible range, and do not benefit from the application of a UV coating. Many modern anti-reflective coatings also block UV.
Scratch resistance
Resists damage to lens surfaces from minor scratches.
Confusing corrective lens industry terminology
Spheric vs. aspheric, atoric, etc.
Lens manufacturers claim that aspheric lenses improve vision over traditional spheric lenses. This statement could be misleading to individuals who do not know that the lenses are being implicitly compared to "a spheric flattened away from best-form for cosmetic reasons". This qualification is necessary since best-form spherics are always better than aspherics for an ophthalmic lens application.[3] Aspherics for corrective lenses are only used to attempt to improve the degradation caused by deviating from best-form sphere resulting from making a flatter lens for cosmetic reasons. The same applies for atoric and bi-aspheric.
It is true that aspheric lenses are used in cameras and binoculars. It would be wrong to assume that this means aspherics/atorics are a sign of good optics in eyewear. Cameras and telescopes use multiple lens elements and have different design criteria. Spectacles are made of only one ophthalmic lens. The best-form spheric lens has been shown to give the best vision. In cases where best-form is not used, such as cosmetic flattening, thinning, or wrap-around sunglasses, an aspheric design can reduce the amount of induced optical distortions.
The problem with aspheric lenses is that they are a broad category. A lens is made of two curved surfaces, and an aspheric lens is a lens where one or both of those surfaces is not spherical. Further research and development is being conducted to determine if the mathematical and theoretical benefits of aspheric lenses can actually lead to better vision correction.
Optical aberrations of the eye lens vs. corrective lens
Optical terms are used to describe error in the eye's lens and the corrective lens. This can cause confusion, since "astigmatism" or "ABBE" has drastically different impact on vision depending on which lens has the error.
Astigmatism disambiguation
Astigmatism of the eye: People prescribed a sphere and a cylinder prescription have astigmatism of the eye and can be given a toric lens to correct it.
Astigmatism of the corrective lens: This phenomenon is called lens-induced oblique astigmatism error (OAE) or power error and is induced when the eye looks through the ophthalmic lens at a point oblique to the optical center (OC). This may become especially evident beyond -6D.
Example: A patient with astigmatism (or no astigmatism) of the eye and a high prescription may notice astigmatism of the lens (OAE) when looking through the corner of their glasses.
Aspheric and atoric disambiguation
An ophthalmic "aspheric lens" specifically refers to a subclass of aspheric lens. Designs referring to "flatter" curves are trading off optical quality for cosmetic appearance. An aspheric lens attempts to correct the error induced by flattening the lens by using a non-spheric lens shape. Typically the design focuses on reducing the error (OAE) across the horizontal and vertical lens axis edges. This can be primarily beneficial to farsighted individuals, whose lenses have a thick center.
An atoric lens design refers to a lens with more complex aspheric lens design. An atoric lens design can address error over more corners of the lens, not just the horizontal and vertical axis.
A toric lens is designed to compensate for the patients with astigmatism. Even though this technically requires an "aspheric" lens, "aspheric" and "atoric" are reserved for lenses which correct errors induced by cosmetic lens flattening.
U.S. legal requirements for prescriptions
In the U.S., laws at the federal and state level govern the provision and effective dates of prescriptions for contact lenses and eyeglasses. (These consumer protection laws grew out of the practice of tying lens purchases to prescription services.) Federal law requires that eyeglass and contact lens prescriptions be given to every consumer, and that the prescriptions be for a minimum of one year. (FTC Section 456.2 “Separation of examination and dispensing” was reviewed in 2004: FTC 2004 review of section 456.2)).
State laws vary. For example, California law also requires prescriptions to be provided to clients whether demanded or not. Eyeglass prescriptions must be for a minimum of 2 years, and contact prescriptions must be for a minimum of 1 year.[10]
See also
- Contact lens
- Dioptre
- Eyeglass prescription
- Lorgnette
- Monocle
- Photochromic lens
- Pince-nez
- Visual acuity
- Tadini, Italian ophthalmologist
References
- ↑ "Progressive Memories & Calculus"
- ↑ "Reading Glasses". Over 40. All about vision. Retrieved 2010-06-14.
- 1 2 Meister, Darryl. "Ophthalmic Lens Design". OptiCampus.com. Retrieved November 12, 2008.
- ↑ Keay L, Friedman DS (2011). "Correcting refractive error in low income countries (editorial)". BMJ. 343: d4793. doi:10.1136/bmj.d4793.
- ↑ J. Gwamuri, B. T. Wittbrodt, N. C. Anzalone, J.M. Pearce. Reversing the Trend of Large Scale and Centralization in Manufacturing: The Case of Distributed Manufacturing of Customizable 3-D-Printable Self-Adjustable Glasses, Challenges in Sustainability 2(1), pp. 30-40 (2014). DOI: 10.12924/cis2014.02010030
- ↑ Zhang M, Zhang R, He M, et al. (2011). "Self correction of refractive error among young people in rural China: results of cross sectional investigation". BMJ. 343: 407. doi:10.1136/bmj.d4767.
- ↑ Code of Federal Regulations Title 21 "Food and Drugs" Sec. 801.410 Use of impact-resistant lenses in eyeglasses and sunglasses
- ↑ Refractive surgery or contact lenses – how and when to decide?, Clinical Optometry, Dove Press, p 68, 10 Nov 2011
- 1 2 Is the sky the limit? MAFO Ophthalmic labs & Industry, April 2009
- ↑ Business and Professions Code Section 2541.1