Bladder exstrophy
| Bladder exstrophy | |
|---|---|
 | |
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 | Q64.1 |
| ICD-9-CM | 753.5 |
| OMIM | 600057 |
| DiseasesDB | 33377 |
| eMedicine | ped/704 |
| MeSH | C12.740.700.132 |
| Orphanet | 93930 |
Bladder exstrophy (also known as Ectopia vesicae) is a congenital anomaly that exists along the spectrum of the exstrophy-epispadias complex and most notably involves protrusion of the urinary bladder through a defect in the abdominal wall. Its presentation is variable, often including abnormalities of the bony pelvis, pelvic floor, and genitalia. The underlying embryologic mechanism leading to bladder exstrophy is unknown, though it is thought to be in part due to failed reinforcement of the cloacal membrane by underlying mesoderm.[1]
Incidence
Occurring at a rate between 1 in 10,000 to 1 in 50,000 [2] with a male-to-female ratio of 2.3-6:1,[3][4][5] bladder exstrophy is relatively rare. For those individuals with bladder exstrophy who maintain their ability to reproduce, the risk of bladder exstrophy in their children is approximately 500-fold greater than the general population.[3]
Presentation
The classic manifestation of bladder exstrophy presents with:
- A defect in the abdominal wall occupied by both the exstrophied bladder as well as a portion of the urethra
- A flattened puborectal sling
- Separation of the pubic symphysis
- Shortening of the pubic ramii
- External rotation of the pelvis.
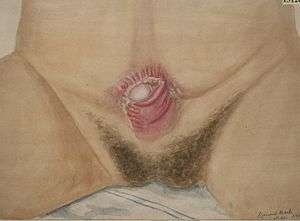
Females frequently have a displaced and narrowed vaginal orifice, a bifid clitoris, and divergent labia.[6]
Prenatal diagnosis
In a small retrospective study of 25 pregnancies five factors were found to be strongly associated with a prenatal diagnosis of bladder exstrophy:
- Inability to visualize the bladder on ultrasound
- A lower abdominal bulge
- A small penis with anteriorly displaced scrotum
- A low set umbilical insertion
- Abnormal widening of the iliac crests
While a diagnosis of bladder exstrophy was made retrospectively in a majority of pregnancies, in only three cases was a prenatal diagnosis made.[7]
Management at birth
Upon delivery, the exposed bladder is irrigated and a non-adherent film is placed to prevent as much contact with the external environment as possible. In the event the child was not born at a medical center with an appropriate exstrophy support team then transfer will likely follow. Upon transfer, or for those infants born at a medical center able to care for bladder exstrophy, imaging may take place in the first few hours of life prior to the child undergoing surgery.[6]
Primary (immediate) closure is indicated only in those patients with a bladder of appropriate size, elasticity, and contractility as those patients are most likely to develop a bladder of adequate capacity after early surgical intervention.[8]
Conditions that are absolute contraindications despite bladder adequacy include duplication of the penis or scrotum and significant bilateral hydronephrosis.
Treatment
Modern therapy is aimed at surgical reconstruction of the bladder and genitalia. Throughout time numerous approaches have been developed, but today only two remain with any frequency:
- In the Modern Staged Repair of Exstrophy (MSRE) the initial step is closure of the abdominal wall, often requiring a pelvic osteotomy. This leaves the patient with penile epispadias and urinary incontinence. At approximately 2–3 years of age the patient then undergoes repair of the epispadias after testosterone stimulation. Finally, bladder neck repair usually occurs around the age of 4–5 years, though this is dependent upon a bladder with adequate capacity and, most importantly, an indication that the child is interested in becoming continent.
- In the Complete Primary Repair of Exstrophy (CPRE) the bladder closure is combined with an epispadias repair, in an effort to decrease costs and morbidity.[9] This technique has, however, led to significant loss of penile and corporal tissue, particularly in younger patients.[10]
Prognosis
The most important criterion for improving long-term prognosis is success of the initial closure.[11][12] If a patient requires more than one closure their chance of continence drops off precipitously with each additional closure - at just two closures the chance of voiding continence is just 17%.[13]
Complications
Even with successful surgery, patients may have long-term complications.[14] Some of the most common include:
References
- ↑ Muecke EC: The role of the cloacal membrane in exstrophy: the first successful experimental study. J Urol 1964; 92:659.
- ↑ Lattimer JK, Smith MJK: Exstrophy closure: a follow up on 70 cases. J Urol 1966; 95:356.
- 1 2 Shapiro E, Jeffs RD, Gearhart JP, Lepor H: Muscarinic cholinergic receptors in bladder exstrophy: insights into surgical management. J Urol 1985; 134:309.
- ↑ Ives E, Coffey R, Carter CO: A family study of bladder exstrophy. J Med Genet 1980; 17:139.
- ↑ Lancaster PAL: Epidemiology of bladder exstrophy: a communication from the International Clearinghouse for Birth Defects monitoring systems. Teratology 1987; 36:221.
- 1 2 Gearhart JP, Mathews R. Exstrophy-epispadias complex. In: Wein AJ, ed. Campbell-Walsh Urology. 10th ed. Philadelphia, Pa: Saunders Elsevier; 2011:chap 124.
- ↑ Gearhart JP, Ben-Chaim J, Jeffs RD, et al: Criteria for the prenatal diagnosis of classic bladder exstrophy. Obstet Gynecol 1995; 85:961.
- ↑ Gearhart JP, Jeffs RD: The bladder exstrophy-epispadias complex. In: Walsh PC, et al ed. Campbell's urology, 7th ed. Philadelphia: WB Saunders; 1998:1939.
- ↑ Grady, Mitchell, 1999. Grady R, Mitchell ME: Complete repair of exstrophy. J Urol 1999; 162:1415.
- ↑ Husmann, Gearhart, 2004. Husmann DA, Gearhart JP: Loss of penile glans and/or corpora following primary repair of bladder exstrophy using the complete penile disassembly technique. J Urol 2004; 172:1696.
- ↑ The importance of a successful initial bladder closure in the surgical management of classical bladder exstrophy: analysis of 144 patients treated at the Johns Hopkins Hospital between 1975 and 1985. 1987 Feb;137(2):258–62.
- ↑ Closure of the exstrophic bladder: an evaluation of the factors leading to its success and its importance on urinary continence. 1989 Aug;142(2 Pt 2):522–4–discussion542–3.
- ↑ Failed exstrophy closure: management and outcome. 2010 Aug;6(4):381–4.
- ↑ Gargollo PC, Borer JG (2007). "Contemporary outcomes in bladder exstrophy". Current Opinion in Urology. 17 (4): 272–80. doi:10.1097/MOU.0b013e3281ddb32f. PMID 17558272.
External links
| Wikimedia Commons has media related to Bladder exstrophy. |