Bethesda system
The Bethesda system (TBS) is a system for reporting cervical or vaginal cytologic diagnoses,[1] used for reporting Pap smear results. It was introduced in 1988,[2] and revised in 1991 [3] and 2001.[1][4][5] The name comes from the location (Bethesda, Maryland) of the conference that established the system.
Additionally, the Bethesda System is used for thyroid cytopathology.
Types of results
Abnormal results include:
- Atypical squamous cells
- Atypical squamous cells of undetermined significance (ASC-US)
- Atypical squamous cells – cannot exclude HSIL (ASC-H)
- Low grade squamous intraepithelial lesion (LGSIL or LSIL)
- High grade squamous intraepithelial lesion (HGSIL or HSIL)
- Squamous cell carcinoma
- Atypical Glandular Cells not otherwise specified (AGC-NOS)
- Atypical Glandular Cells, suspicious for AIS or cancer (AGC-neoplastic)
- Adenocarcinoma in situ (AIS)
The results are calculated differently following fine needle aspiration of thyroid nodules.
Squamous cell abnormalities
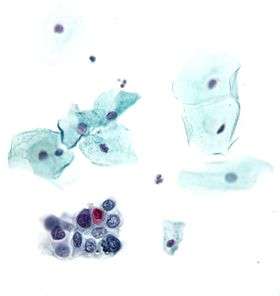
LSIL: low-grade squamous intraepithelial lesion

Low-grade squamous intraepithelial lesion (LSIL or LGSIL) indicates possible cervical dysplasia. LSIL usually indicates mild dysplasia (CIN 1), more than likely caused by a human papillomavirus infection. It is usually diagnosed following a Pap smear.
CIN 1 is the most common and most benign form of cervical intraepithelial neoplasia and usually resolves spontaneously within two years. Because of this, LSIL results can be managed with a simple "watch and wait" philosophy. However, because there is a 12–16% chance of progression to more severe dysplasia, the physician may want to follow the results more aggressively by performing a colposcopy with biopsy.[6] If the dysplasia progresses, treatment may be necessary. Treatment involves removal of the affected tissue, which can be accomplished by LEEP, cryosurgery, cone biopsy, or laser ablation.
HSIL: high-grade squamous intraepithelial lesion
High-grade squamous intraepithelial lesion (HSIL or HGSIL) indicates moderate or severe cervical intraepithelial neoplasia or carcinoma in situ. It is usually diagnosed following a Pap test. In some cases these lesions can lead to invasive cervical cancer, if not followed appropriately.
HSIL does not mean that cancer is present. Of all women with HSIL results, 2%[7] or less[8] have invasive cervical cancer at that time, however about 20% would progress to having invasive cervical cancer without treatment.[9] To combat this progression, HSIL is usually followed by an immediate colposcopy with biopsy to sample or remove the dysplastic tissue. This tissue is sent for pathology testing to assign a histologic classification that is more definitive than a Pap smear result (which is a cytologic finding). HSIL generally corresponds to the histological classification of CIN 2 or 3.
HSIL treatment involves the removal or destruction of the affected cells, usually by LEEP. Other methods include cryotherapy, cautery, or laser ablation, but none are performed on pregnant women for fear of disrupting the pregnancy.[10] Any of these procedures is 85% likely to cure the problem.
Glandular cell abnormalities
Adenocarcinoma

Adenocarcinoma can arise from the endocervix, endometrium and extrauterine sites.
AGC
AGC, formerly AGUS, is an acronym for atypical glandular cells of undetermined significance.[11] Renamed AGC to avoid confusion with ASCUS.[1]
The management of AGC is colposcopy with or without an endometrial biopsy.
See also
References
- 1 2 3 Apgar BS, Zoschnick L, Wright TC (November 2003). "The 2001 Bethesda System terminology". Am Fam Physician. 68 (10): 1992–8. PMID 14655809.
- ↑ "The 1988 Bethesda System for reporting cerval/vaginal cytologic diagnoses: developed and approved at the National Cancer Institute workshop in Bethesda, MD, December 12–13, 1988". Diagn. Cytopathol. 5 (3): 331–4. 1989. doi:10.1002/dc.2840050318. PMID 2791840.
- ↑ Broder S (1992). "The Bethesda System for Reporting Cervical/Vaginal Cytologic Diagnoses—Report of the 1991 Bethesda Workshop". JAMA. 267: 1892. doi:10.1001/jama.1992.03480140014005.
- ↑ Nayar R, Solomon D. Second edition of 'The Bethesda System for reporting cervical cytology' – Atlas, website, and Bethesda interobserver reproducibility project. CytoJournal [serial online] 2004 [cited 2011 Apr 17];1:4. Available from: http://www.cytojournal.com/text.asp?2004/1/1/4/41272
- ↑ Solomon D, Davey D, Kurman R, et al. (April 2002). "The 2001 Bethesda System: terminology for reporting results of cervical cytology". JAMA. 287 (16): 2114–9. doi:10.1001/jama.287.16.2114. PMID 11966386.
- ↑ Wright TC Jr, Massad LS, Dunton CJ, Spitzer M, Wilkinson EJ, Solomon D (Oct 2007). "2006 consensus guidelines for the management of women with abnormal cervical cancer screening tests". Am J Obstet Gynecol. 197 (4): 346–55. doi:10.1016/j.ajog.2007.07.047.
- ↑ Massad LS; Collins YC; Meyer PM. Biopsy correlates of abnormal cervical cytology classified using the Bethesda system. Gynecologic Oncology. 2001 Sep;82(3):516-22.
- ↑ Melnikow J, Nuovo J, Willan AR, Chan BK, Howell LP. Natural history of cervical squamous intraepithelial lesions: a meta-analysis. Obstetric Gynecology. 1998 Oct;92(4 Pt 2):727-35.
- ↑ McIndoe WA; McLean MR; Jones RW; Mullins PR. The invasive potential of carcinoma in situ of the cervix. Obstetric Gynecology. 1984 Oct;64(4):451-8.
- ↑ Wright TC Jr; Massad LS; Dunton CJ; Spitzer M; Wilkinson EJ; Solomon D. 2006 consensus guidelines for the management of women with abnormal cervical cancer screening tests. American Journal of Obstetric Gynecology. 2007 Oct;197(4):346-55.
- ↑ AGUS at eMedicine Dictionary