Modes of mechanical ventilation
Modes of mechanical ventilation are one of the most important aspects of the usage of mechanical ventilation. The mode refers to the method of inspiratory support. In general, mode selection is based on clinician familiarity and institutional preferences, since there is a paucity of evidence indicating that the mode affects clinical outcome. The most frequently used forms of volume-limited mechanical ventilation are intermittent mandatory ventilation (IMV) and continuous mandatory ventilation (CMV).[1] There have been substantial changes in the nomenclature of mechanical ventilation over the years, but more recently it has become standardized by many respirology and pulmonology groups.[2][3] Writing a mode is most proper in all capital letters with a dash between the cycle and the strategy (i.e. PC-IMV, or VC-MMV etc.)
Taxonomy for mechanical ventilation
The taxonomy is a logical classification system based on 10 maxims of ventilator design[4]
10 maxims
- A breath is one cycle of positive flow (inspiration) and negative flow (expiration) defined in terms of the flow-time curve. Inspiratory time is defined as the period from the start of positive flow to the start of negative flow. Expiratory time is defined as the period from the start of expiratory flow to the start of inspiratory flow. The flow-time curve is the basis for many variables related to ventilator settings.
- A breath is assisted if the ventilator does work on the patient. An assisted breath is one for which the ventilator does some portion of the work of breathing. For constant flow inflation, work is defined as inspiratory pressure multiplied by tidal volume. Therefore, an assisted breath is identified as a breath for which airway pressure (displayed on the ventilator) rises above baseline during inspiration. An unassisted breath is one for which the ventilator simply provides the inspiratory flow demanded by the patient and pressure stays constant throughout the breath.
- A ventilator assists breathing using either pressure control or volume control based on the equation of motion for the respiratory system. Providing assistance means doing work on the patient, which is accomplished by controlling either pressure or volume. A simple mathematical model describing this fact is known as the equation of motion for the passive respiratory system:
Pressure = (Elastance × Volume) + (Resistance × Flow)
In this equation, pressure, volume, and flow are all continuous functions of time. Pressure is actually a pressure difference across the system (e.g., transrespiratory pressure defined as pressure at the airway opening minus pressure on the body surface). Elastance (defined as the change in pressure divided by the associated change in volume; the reciprocal of compliance) and resistance (defined as a change in pressure divided by the associated change in flow) are parameters assumed to remain constant during a breath.Volume control (VC) means that both volume and flow are preset prior to inspiration. In other words, the right hand side of the equation of motion remains constant while pressure changes with changes in elastance and resistance.
Pressure control (PC) means that inspiratory pressure is preset as either a constant value or it is proportional to the patient’s inspiratory effort. In other words, the left-hand side of the equation of motion remains constant while volume and flow change with changes in elastance and resistance.
Time control (TC) means that, in some rare situations, none of the main variables (pressure, volume, or flow) are preset. In this case only the inspiratory and expiratory times are preset. - Breaths are classified by the criteria that trigger (start) and cycle (stop) inspiration. The start of inspiration is called the trigger event. The end of inspiration is called the cycle event.
- Trigger and cycle events can be initiated by the patient or the machine. Inspiration can be patient triggered or patient cycled by a signal representing inspiratory effort. Inspiration may also be machine triggered or machine cycled by preset ventilator thresholds.
Patient triggering means starting inspiration based on a patient signal independent of a machine trigger signal. Machine triggering means starting inspiratory flow based on a signal from the ventilator, independent of a patient trigger signal. Patient cycling means ending inspiratory time based on signals representing the patient determined components of the equation of motion, (ie, elastance or resistance and including effects due to inspiratory effort). Flow cycling is a form of patient cycling because the rate of flow decay to the cycle threshold is determined by patient mechanics. Machine cycling means ending inspiratory time independent of signals representing the patient determined components of the equation of motion.
- Breaths are classified as spontaneous or mandatory based on both the trigger and cycle events. A spontaneous breath is a breath for which the patient both triggers and cycles the breath. A spontaneous breath may occur during a mandatory breath (e.g. Airway Pressure Release Ventilation). A spontaneous breath may be assisted or unassisted. A mandatory breath is a breath for which the machine triggers and/or cycles the breath. A mandatory breath can occur during a spontaneous breath (e.g., High Frequency Jet Ventilation). A mandatory breath is, by definition, assisted.
- There are 3 breath sequences: Continuous mandatory ventilation (CMV), Intermittent Mandatory Ventilation (IMV), and Continuous Spontaneous Ventilation (CSV). A breath sequence is a particular pattern of spontaneous and/or mandatory breaths. The 3 possible breath sequences are: continuous mandatory ventilation, (CMV, spontaneous breaths are not allowed between mandatory breaths), intermittent mandatory ventilation (IMV, spontaneous breaths may occur between mandatory breaths), and continuous spontaneous ventilation (CSV, all breaths are spontaneous).
- There are 5 basic ventilatory patterns: VC-CMV, VC-IMV, PC-CMV, PC-IMV, and PC-CSV. The combination VC-CSV is not possible because volume control implies machine cycling and machine cycling makes every breath mandatory, not spontaneous. A sixth pattern, TC-IMV is possible but rare.
- Within each ventilatory pattern there are several variations that can be distinguished by their targeting scheme(s). A targeting scheme is a description of how the ventilator achieves preset targets. A target is a predetermined goal of ventilator output. Examples of within-breath targets include inspiratory flow or pressure and rise time (set-point targeting), tidal volume (dual targeting) and constant of proportionality between inspiratory pressure and patient effort (servo targeting). Examples of between-breath targets and targeting schemes include average tidal volume (for adaptive targeting), percent minute ventilation (for optimal targeting) and combined PCO2, volume, and frequency values describing a “zone of comfort” (for intelligent targeting, e.g., SmartCarePS or IntelliVent-ASV). The targeting scheme (or combination of targeting schemes) is what distinguishes one ventilatory pattern from another. There are 7 basic targeting schemes that comprise the wide variety seen in different modes of ventilation:
Set-point: A targeting scheme for which the operator sets all the parameters of the pressure waveform (pressure control modes) or volume and flow waveforms (volume control modes).
Dual: A targeting scheme that allows the ventilator to switch between volume control and pressure control during a single inspiration.
Bio-variable: A targeting scheme that allows the ventilator to automatically set the inspiratory pressure or tidal volume randomly to mimic the variability observed during normal breathing.
Servo: A targeting scheme for which inspiratory pressure is proportional to inspiratory effort.
Adaptive: A targeting scheme that allows the ventilator to automatically set one target (eg, pressure within a breath) to achieve another target (eg, average tidal volume over several breaths).
Optimal: A targeting scheme that automatically adjusts the targets of the ventilatory pattern to either minimize or maximize some overall performance characteristic (eg, minimize the work rate done by the ventilatory pattern).
Intelligent: A targeting scheme that uses artificial intelligence programs such as fuzzy logic, rule based expert systems, and artificial neural networks. - A mode of ventilation is classified according to its control variable, breath sequence, and targeting scheme(s). The preceding 9 maxims create a theoretical foundation for a taxonomy of mechanical ventilation. The taxonomy is based on these theoretical constructs and has 4 hierarchical levels:
- Control Variable (Pressure or Volume, for the primary breath)
- Breath Sequence (CMV, IMV, or CSV)
- Primary Breath Targeting Scheme (for CMV or CSV)
- Secondary Breath Targeting Scheme (for IMV)
The “primary breath” is either the only breath there is (mandatory for CMV and spontaneous for CSV) or it is the mandatory breath in IMV. The targeting schemes can be represented by single, lower case letters: set-point = s, dual = d, servo = r, bio-variable = b, adaptive = a, optimal = o, intelligent = i. A tag is an abbreviation for a mode classification, such as PC-IMVs,s. Compound tags are possible, eg, PC-IMVoi,oi.
How modes are classified
Step 1: Identify the primary breath control variable. If inspiration starts with a preset inspiratory pressure, or if pressure is proportional to inspiratory effort, then the control variable is pressure. If inspiration starts with a preset tidal volume and inspiratory flow, then the control variable is volume. If neither is true, the control variable is time.
Step 2: Identify the breath sequence. Determine whether trigger and cycle events are patient or machine determined. Then, use this information to determine the breath sequence.
Step 3: Identify the targeting schemes for the primary breaths and (if applicable) secondary breaths.
Example mode classification
Mode Name: A/C Volume Control (Covidien PB 840)
- Inspiratory volume and flow are preset, so the control variable is volume.
- Every breath is volume cycled, which is a form of machine cycling. Any breath for which inspiration is machine cycled is classified as a mandatory breath. Hence, the breath sequence is continuous mandatory ventilation.
- The operator sets all the parameters of the volume and flow waveforms so the targeting scheme is set-point. Thus, the mode is classified as volume control continuous mandatory ventilation with set-point targeting (VC-CMVs).
Mode Name: SIMV Volume Control Plus (Covidien PB 840)
- The operator sets the tidal volume but not the inspiratory flow. Because setting volume alone (like setting flow alone) is a necessary but not sufficient criterion for volume control, the control variable is pressure.
- Spontaneous breaths are allowed between mandatory breaths so the breath sequence is IMV.
- The ventilator adjusts inspiratory pressure between breaths to achieve an average preset tidal volume, so the targeting scheme is adaptive. The mode tag is PC-IMVa,s.
Descriptions of common modes
Assist mode, control mode, and assist-control mode
A basic distinction in mechanical ventilation is whether each breath is initiated by the patient (assist mode) or by the machine (control mode). Dynamic hybrids of the two (assist-control modes) are also possible, and control mode without assist is now mostly obsolete.
Airway pressure release ventilation
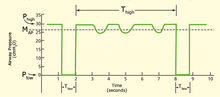
Airway pressure release ventilation is a time-cycled alternant between two levels of positive airway pressure, with the main time on the high level and a brief expiratory release to facilitate ventilation.[5]
Airway pressure release ventilation is usually utilized as a type of inverse ratio ventilation. The exhalation time (Tlow) is shortened to usually less than one second to maintain alveoli inflation. In the basic sense, this is a continuous pressure with a brief release. APRV currently the most efficient conventional mode for lung protective ventilation.[6]
Different perceptions of this mode may exist around the globe. While 'APRV' is common to users in North America, a very similar mode, biphasic positive airway pressure (BIPAP), was introduced in Europe.[7] The term APRV has also been used in American journals where, from the ventilation characteristics, BIPAP would have been perfectly good terminology.[8] But BiPAP(tm) is a trademark for a noninvasive ventilation mode in a specific ventilator (Respironics Inc.).
Other manufacturers have followed with their own brand names (BILEVEL, DUOPAP, BIVENT). Although similar in modality, these terms describe how a mode is intended to inflate the lung, rather than defining the characteristics of synchronization or the way spontaneous breathing efforts are supported.
Intermittent mandatory ventilation has not always had the synchronized feature, so the division of modes were understood to be SIMV (synchronized) vs IMV (not-synchronized). Since the American Association for Respiratory Care established a nomenclature of mechanical ventilation the "synchronized" part of the title has been dropped and now there is only IMV.
Mandatory minute ventilation
Mandatory minute ventilation (MMV) allows spontaneous breathing with automatic adjustments of mandatory ventilation to the meet the patient’s preset minimum minute volume requirement. If the patient maintains the minute volume settings for VT x f, no mandatory breaths are delivered.
If the patient's minute volume is insufficient, mandatory delivery of the preset tidal volume will occur until the minute volume is achieved. The method for monitoring whether or not the patient is meeting the required minute ventilation (VE) differs by ventilator brand and model, but, in general, there is a window of monitored time, and a smaller window checked against the larger window (i.e., in the Dräger Evita® line of mechanical ventilators there is a moving 20-second window, and every 7 seconds the current tidal volume and rate are measured) to decide whether a mechanical breath is needed to maintain the minute ventilation.
MMV is an optimal mode for weaning in neonatal and pediatric populations and has been shown to reduce long-term complications related to mechanical ventilation.[9]
Pressure-regulated volume control
Pressure-regulated volume control is an IMV based mode. Pressure-regulated volume control utilizes pressure-limited, volume-targeted, time-cycled breaths that can be either ventilator- or patient-initiated.
The peak inspiratory pressure delivered by the ventilator is varied on a breath-to-breath basis to achieve a target tidal volume that is set by the clinician.
For example, if a target tidal volume of 500 mL is set but the ventilator delivers 600 mL, the next breath will be delivered with a lower inspiratory pressure to achieve a lower tidal volume. Though PRVC is regarded as a hybrid mode because of its tidal-volume (VC) settings and pressure-limiting (PC) settings fundamentally PRVC is a pressure-control mode with adaptive targeting.
Continuous positive airway pressure
Continuous positive airway pressure (CPAP) is a non-invasive positive pressure mode of ventilation (NPPV). CPAP is a pressure applied at the end of exhalation to keep the alveoli open and not fully deflate. This mechanism for maintaining inflated alveoli helps increase partial pressure of oxygen in arterial blood, an appropriate increase in CPAP increases the PaO2.
Bilevel positive airway pressure
Bilevel positive airway pressure (BPAP) is a mode used during noninvasive positive pressure ventilation (NPPV). First used in 1988 by Professor Benzer in Austria,[10] it delivers a preset inspiratory positive airway pressure (IPAP) and expiratory positive airway pressure (EPAP). BPAP can be described as a Continuous Positive Airway Pressure system with a time-cycled change of the applied CPAP level.[11] CPAP, BPAP and other non-invasive ventilation modes have been shown to be effective management tools for chronic obstructive pulmonary disease and acute respiratory failure.[12]
Often BPAP is incorrectly referred to as "BiPAP". BiPAP® is the name of a portable ventilator manufactured by Respironics Corporation; it is just one of many ventilators that can deliver BPAP.
High-frequency ventilation (Active)
The term active refers to the ventilator's forced expiratory system. In a HFV-A scenario, the ventilator uses pressure to apply an inspiratory breath and then applies an opposite pressure to force an expiratory breath. In high-frequency oscillatory ventilation (sometimes abbreviated HFOV) the oscillation bellows and piston force positive pressure in and apply negative pressure to force an expiration.[13]
High-frequency ventilation (Passive)
The term passive refers to the ventilator's non-forced expiratory system. In a HFV-P scenario, the ventilator uses pressure to apply an inspiratory breath and then returns to atmospheric pressure to allow for a passive expiration. This is seen in High-Frequency Jet Ventilation, sometimes abbreviated HFJV.
Volume guarantee
Volume guarantee an additional parameter available in many types of ventilators that allows the ventilator to change its inspiratory pressure setting to achieve a minimum tidal volume. This is utilized most often in neonatal patients who need a pressure controlled mode with a consideration for volume control to minimize volutrauma.
Spontaneous breathing and support settings
Positive-end expiratory pressure
Positive end expiratory pressure (PEEP) is pressure applied upon expiration. PEEP is applied using either a valve that is connected to the expiratory port and set manually or a valve managed internally by a mechanical ventilator.
PEEP is a pressure that an exhalation has to bypass, in effect causing alveoli to remain open and not fully deflate. This mechanism for maintaining inflated alveoli helps increase partial pressure of oxygen in arterial blood, and an increase in PEEP increases the PaO2.[14]
Pressure support
Pressure support is a spontaneous mode of ventilation also named Pressure Support Ventilation (PSV). The patient initiates every breath and the ventilator delivers support with the preset pressure value. With support from the ventilator, the patient also regulates their own respiratory rate and their tidal volume.
In Pressure Support, the set inspiratory pressure support level is kept constant and there is a decelerating flow. The patient triggers all breaths. If there is a change in the mechanical properties of the lung/thorax and patient effort, the delivered tidal volume will be affected. The user must then regulate the pressure support level to obtain desired ventilation.[15][16]
Pressure support improves oxygenation,[17] ventilation and decreases work of breathing.
Also see adaptive support ventilation.
Other ventilation modes and strategies
Closed loop systems
Adaptive Support Ventilation
Adaptive Support Ventilation is the only commercially available closed-loop mode of mechanical ventilation to date that uses "optimal targeting". This targeting scheme was first described by Tehrani in 1991,[18][19] and was designed to minimize the work rate of breathing, mimic natural breathing, stimulate spontaneous breathing, and reduce weaning time.[20]
Automatic Tube Compensation
Automatic Tube Compensation (ATC) is the simplest example of a computer-controlled targeting system on a ventilator. It is a form of servo targeting.
The goal of ATC is to support the resistive work of breathing through the artificial airway
Neurally Adjusted Ventilatory Assist
Neurally Adjusted Ventilatory Assist (NAVA) is adjusted by a computer (servo) and is similar to ATC but with more complex requirements for implementation.
In terms of patient-ventilator synchrony, NAVA supports both resistive and elastic work of breathing in proportion to the patient’s inspiratory effort
Proportional Assist Ventilation
Proportional assist ventilation (PAV) is another servo targeting based mode in which the ventilator guarantees the percentage of work regardless of changes in pulmonary compliance and resistance.[21]
The ventilator varies the tidal volume and pressure based on the patient's work of breathing. The amount it delivers is proportional to the percentage of assistance it is set to give.
PAV, like NAVA, supports both restrictive and elastic work of breathing in proportion to the patient’s inspiratory effort.
Liquid ventilation
Liquid ventilation is a technique of mechanical ventilation in which the lungs are insufflated with an oxygenated perfluorochemical liquid rather than an oxygen-containing gas mixture. The use of perfluorochemicals, rather than nitrogen, as the inert carrier of oxygen and carbon dioxide offers a number of theoretical advantages for the treatment of acute lung injury, including:
- Reducing surface tension by maintaining a fluid interface with alveoli
- Opening of collapsed alveoli by hydraulic pressure with a lower risk of barotrauma
- Providing a reservoir in which oxygen and carbon dioxide can be exchanged with pulmonary capillary blood
- Functioning as a high-efficiency heat exchanger
Despite its theoretical advantages, efficacy studies have been disappointing and the optimal clinical use of LV has yet to be defined.[22]
Total liquid ventilation
In total liquid ventilation (TLV), the entire lung is filled with an oxygenated PFC liquid, and a liquid tidal volume of PFC is actively pumped into and out of the lungs. A specialized apparatus is required to deliver and remove the relatively dense, viscous PFC tidal volumes, and to extracorporeally oxygenate and remove carbon dioxide from the liquid.[23][24][25]
Partial liquid ventilation
In partial liquid ventilation (PLV), the lungs are slowly filled with a volume of PFC equivalent or close to the FRC during gas ventilation. The PFC within the lungs is oxygenated and carbon dioxide is removed by means of gas breaths cycling in the lungs by a conventional gas ventilator.[26]
See also
References
- ↑ Esteban A, Anzueto A, Alía I, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med 2000; 161:1450.
- ↑ Donn SM (2009). "Neonatal ventilators: how do they differ?". J Perinatol. 29 Suppl 2: S73–8. doi:10.1038/jp.2009.23. PMID 19399015.
- ↑ Chatburn RL, Volsko TA, Hazy J, Harris LN, Sanders S (2011). "Determining the Basis for a Taxonomy of Mechanical Ventilation.". Respir Care. 57 (4): 514–24. doi:10.4187/respcare.01327. PMID 22004898.
- ↑ Chatburn, Robert; El-Khatib, Mohamad; Mireles-Cabodevila, Eduardo (2014). "A taxonomy for mechanical ventilation: 10 fundamental maxims.". Respiratory Care: 1747–1763.
- ↑ Dietrich Henzler (2011). "What on earth is APRV?". Critical Care. London, England. 15 (1): 115. doi:10.1186/cc9419. PMC 3222047
 . PMID 21345265.
. PMID 21345265. - ↑ Adrian A. Maung & Lewis J. Kaplan (July 2011). "Airway pressure release ventilation in acute respiratory distress syndrome". Critical Care Clinics. 27 (3): 501–509. doi:10.1016/j.ccc.2011.05.003. PMID 21742214.
- ↑ M. Baum, H. Benzer, C. Putensen, W. Koller & G. Putz (September 1989). "[Biphasic positive airway pressure (BIPAP)--a new form of augmented ventilation]". Der Anaesthesist. 38 (9): 452–458. PMID 2686487.
- ↑ C. Putensen, S. Zech, H. Wrigge, J. Zinserling, F. Stuber, T. Von Spiegel & N. Mutz (July 2001). "Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury". American Journal of Respiratory and Critical Care Medicine. 164 (1): 43–49. doi:10.1164/ajrccm.164.1.2001078. PMID 11435237.
- ↑ Scott O. Guthrie, Chris Lynn, Bonnie J. Lafleur, Steven M. Donn & William F. Walsh (October 2005). "A crossover analysis of mandatory minute ventilation compared to synchronized intermittent mandatory ventilation in neonates". Journal of perinatology : official journal of the California Perinatal Association. 25 (10): 643–646. doi:10.1038/sj.jp.7211371. PMID 16079905.
- ↑ Benzer H (1988) Ventilatory support by intermittent changes in PEEP levels. 4th European Congress on Intensive Care Medicine. Baveno-Stresa
- ↑ C. Hormann, M. Baum, C. Putensen, N. J. Mutz & H. Benzer (January 1994). "Biphasic positive airway pressure (BIPAP)--a new mode of ventilatory support". European Journal of Anaesthesiology. 11 (1): 37–42. PMID 8143712.
- ↑ M. A. Levitt (November 2001). "A prospective, randomized trial of BiPAP in severe acute congestive heart failure". The Journal of Emergency Medicine. 21 (4): 363–369. doi:10.1016/s0736-4679(01)00385-7. PMID 11728761.
- ↑ Allardet-Servent J (2011). "High-frequency oscillatory ventilation in adult patients with acute respiratory distress syndrome: Where do we stand and where should we go?". Crit Care Med. 39 (12): 2761–2. doi:10.1097/CCM.0b013e31822a5c35. PMID 22094505.
- ↑ D. P. Schuster, M. Klain & J. V. Snyder (October 1982). "Comparison of high frequency jet ventilation to conventional ventilation during severe acute respiratory failure in humans". Critical Care Medicine. 10 (10): 625–630. doi:10.1097/00003246-198210000-00001. PMID 6749433.
- ↑ MAQUET, "Modes of ventilation in SERVO-i, invasive and non-invasive", 2008 MAQUET Critical Care AB, Order No 66 14 692
- ↑ MAQUET, "Modes of ventilation in SERVO-s, invasive and non-invasive", 2009 MAQUET Critical Care AB, Order No 66 61 131
- ↑ Spieth PM, Carvalho AR, Güldner A, et al. (April 2011). "Pressure support improves oxygenation and lung protection compared to pressure-controlled ventilation and is further improved by random variation of pressure support". Critical Care Medicine. 39 (4): 746–55. doi:10.1097/CCM.0b013e318206bda6. PMID 21263322.
- ↑ Tehrani FT. Method and apparatus for controlling an artificial respiratory. US patent 4,986,268, issued January 22, 1991.
- ↑ Tehrani FT. Automatic control of an artificial respirator. Proc IEEE EMBS Conf 1991;13:1738-1739.
- ↑ Tehrani FT. Automatic control of mechanical ventilation. Part 2: The existing techniques and future trends J Clin Monit Comput 2008; 22(6):417-424.
- ↑ Younes M. Proportional assist ventilation, a new approach to ventilatory support. Theory. Am Rev Respir Dis 1992; 145(1):114-120.
- ↑ Degraeuwe PL, Vos GD, Blanco CE (1995). "Perfluorochemical liquid ventilation: from the animal laboratory to the intensive care unit.". Int J Artif Organs. 18 (10): 674–83. PMID 8647601.
- ↑ Norris MK, Fuhrman BP, Leach CL (1994). "Liquid ventilation: it's not science fiction anymore.". AACN Clin Issues Crit Care Nurs. 5 (3): 246–54. PMID 7780839.
- ↑ Greenspan JS (1996). "Physiology and clinical role of liquid ventilation therapy.". J Perinatol. 16 (2 Pt 2 Su): S47–52. PMID 8732549.
- ↑ Dirkes S (1996). "Liquid ventilation: new frontiers in the treatment of ARDS.". Crit Care Nurse. 16 (3): 53–8. PMID 8852261.
- ↑ Cox CA, Wolfson MR, Shaffer TH (1996). "Liquid ventilation: a comprehensive overview.". Neonatal Netw. 15 (3): 31–43. PMID 8715647.