Renal stone formation in space

Renal stone formation and passage during space flight can potentially pose a severe risk to crew member health and safety and could affect mission outcome. While the renal stones are routinely and successfully treated on Earth, the occurrence of these during space flight can prove to be problematic.[1]
Causes and countermeasures
Causes

Several factors contribute to the formation of renal stones in space. Dietary changes, bone metabolism, dehydration, increased salt intake as well as decreased urine volumes and increased urine saturation are all possible causes of renal stone formation.[2] It has been noted that spaceflight-induced changes in urine biochemistry are conducive for stone formation.[1]
Other possible causes include:
- increased urinary pH
- history of or predisposition to stone formation
- inflight food stability[3]
- preservation of food using salt
- quantity of onboard water supply[4]
- limited nutritional sources
- increased diet of animal protein
The most common renal stone is calcium oxalate and is usually caused by treatable metabolic disorders of hypercalcuria (increased calcium levels in the urine). These stones cause pain with passage and blockage and have been known to recur.[2]
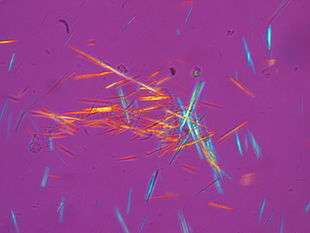
Uric acid stones have similar characteristics as the calcium oxalate stones, but occur much more rarely (approximately 5% of all renal stones). Since they are translucent, they cannot be seen by radiographs.[2]
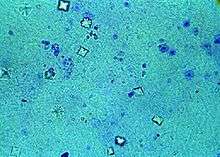
Struvite stones are generated by infections of urease-containing microorganisms that are capable of hydrolyzing the urea in the urine to carbon dioxide and ammonia. Struvite stones can form when urinary pH rises above 7.2, can fill the renal collection system, and can erode into the renal tissue.[2]
Cystine stones, caused by hereditary cystinuria, begin forming in childhood and can grow large enough to fill the renal collection system.[2]
Calcium phosphate stones, or otherwise called brushite, are caused by high urine pH and a supersaturation of calcium phosphate salt in the urine.[2]
Countermeasures
It is more cost effective to prevent stone formation during a mission than is it to treat it. Increased fluid intake will increase urine volume and dilute the stone-forming salts to below the upper risk levels.[5] Avoiding foods that are high in fat and high in oxalate (nuts, pepper, chocolate, rhubarb, spinach, dark green vegetables, fruits) can help reduce hyperoxaluria (excessive urinary excretion of oxalate). Reducing the amount of meats and other purine-containing foods suppresses hyperuricosuria (increased amounts of uric acid in the urine).[6]
Oral alkali (such as potassium citrate) raises the urine's pH and helps suppress calcium oxalate crystal formation. This also works by binding the calcium to form calcium citrate (a crystal growth and aggregation inhibitor). Studies have also shown an additive effect of potassium citrate.[6] The ingestion of potassium citrate has been associated with increased bone density[7] as well as the prevention of bone loss by providing an alkali load averting the bone resorbing effect of sodium chloride excess.[8] Potassium citrate has also been shown to reduce bone loss in postmenopausal women[9] and also improves calcium balance in patients with distal renal tubular acidosis[10]
On the ground
Bed rest studies[11] are used as ground-based analogs to space flight environments. During these studies, the rate of bone loss and subsequent urine composition are similar to those observed in space. A recent ground-based study tested the effectiveness of potassium-magnesium citrate (similar to the currently used potassium citrate) as a countermeasure for renal stones.[12]
Computer based simulations
The Integrated Medical Model (IMM)[13] group at Glenn Research Center in Ohio has been analyzing and optimizing data gathered on renal stone formation since late 2008.
In space
Since the risk of renal stone formation could, as has, result in the loss of a crew member to a mission,[1] regular testing is conducted. To date, there has been only one inflight instance of renal stone formation (described in detail in Valentin Lebedev's book, Diary of a Cosmonaut: Two hundred eleven days in space).[1]
Skylab
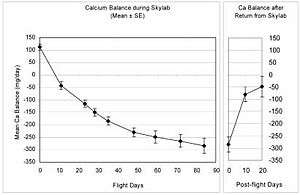
The Skylab missions were the first missions that extended past several days in duration. Testing during these missions showed that calcium excretion increased early in flight and almost exceeded the upper threshold for normal excretion.[15]
Shuttle missions

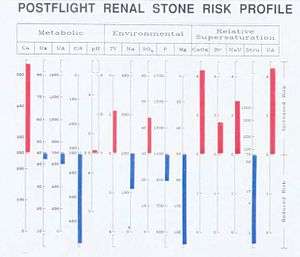
Investigations of environmental and biochemical renal stone formation risk factors on short and long duration Shuttle missions showed that an increased risk of calcium oxalate and uric acid stone formation was evident immediately post-flight.[16] Nutrition, urinary pH and volume output were found to be the largest contributing factors for these formations.[17] During longer Shuttle missions, the risk for stone formation rapidly increases throughout the mission and persists after landing.[18]
Figures 4-2a and 4-2b show the relative risks of stone formation in a representative crewmember of a space shuttle flight. A retrospective medical chart review for stone formation in U.S. astronauts reported that 12 different astronauts reported 14 cases of renal stone formations with 9 of those instances occurring in the postflight period.[15]
Shuttle-Mir missions
Data gathered during 129- to 208-day Shuttle-Mir missions suggest that the spaceflight environment and subsequent return to Earth change the composition of the astronauts' urine and promoted the formation of renal stones.[19] This data shows that there was an increased risk for calcium oxalate and calcium phosphate stones during flight, and an increased risk for calcium oxalate and uric acid stones immediately after flight. This post-flight stone development could be attributed to low urine volumes and higher urinary pH.[15]
International Space Station (ISS)
Flight experiment 96-E057, Renal stone risk during spaceflight: Assessment and countermeasure evaluation,[20] was conducted on Expeditions 3, 4, 5, 6, 8, 11, 12, 13, and 14. The aim of this experiment was to evaluate the in-flight effectiveness of potassium citrate as a countermeasure against the formation of renal stones during long duration space flight. The results of this experiment described the renal stone forming potential in crewmembers as a function of time in space as well as the stone forming potential during the postflight period.[15][21]
Future exploration missions
Exploration missions pose an extra threat to mission outcome and crewmember health and safety due to the longer duration of the mission as well as the greater distances traveled. Since acute illness caused by the formation and passage of renal stones could cause the loss of a crewmember to a mission, it is critical that valid countermeasures are put in place before exploration missions begin.[15]
Table 4-4 outlines specific scenarios and time considerations for exploration missions.
| Duration Length | Mission Location | Transit Time To Location (in days) | Length Of Stay (in days) | Transit Time Back To Earth (in days) |
|---|---|---|---|---|
| Short | Moon | 3 | 8 | 3 |
| Long | Moon | 5 | 170 | 5 |
| Short | Mars | 162 | 40 | 162 |
| Long | Mars | 189 | 540 | 189 |
References
- 1 2 3 4 Risk of Renal Stone Formation (PDF). Human Research Program: Human Health Countermeasures Element (HRP-47060). NASA. March 2008. p. 3.
- 1 2 3 4 5 6 Risk of Renal Stone Formation (PDF). Human Research Program: Human Health Countermeasures Element (HRP-47060). NASA. March 2008. p. 4.
- ↑ http://www.nasa.gov/centers/johnson/slsd/about/divisions/hefd/facilities/space-food.html[]
- ↑ http://www.water-technology.net/projects/iss_water_recovery/[]
- ↑ Whitson, PA; Pietrzyk, RA; Sams, CF (2001). "Urine volume and its effects on renal stone risk in astronauts". Aviation, space, and environmental medicine. 72 (4): 368–72. PMID 11318017.
- 1 2 Risk of Renal Stone Formation (PDF). Human Research Program: Human Health Countermeasures Element (HRP-47060). NASA. March 2008. p. 5.
- ↑ Pak, CY; Peterson, RD; Poindexter, J (2002). "Prevention of spinal bone loss by potassium citrate in cases of calcium urolithiasis". The Journal of Urology. 168 (1): 31–4. doi:10.1016/s0022-5347(05)64825-2. PMID 12050486.
- ↑ Sellmeyer, D. E. (2002). "Potassium Citrate Prevents Increased Urine Calcium Excretion and Bone Resorption Induced by a High Sodium Chloride Diet". Journal of Clinical Endocrinology & Metabolism. 87 (5): 2008. doi:10.1210/jc.87.5.2008.
- ↑ Marangella, M.; Di Stefano, M.; Casalis, S.; Berutti, S.; d’Amelio, P.; Isaia, G. C. (2004). "Effects of Potassium Citrate Supplementation on Bone Metabolism". Calcified Tissue International. 74 (4): 330–5. doi:10.1007/s00223-003-0091-8. PMID 15255069.
- ↑ Preminger, GM; Sakhaee, K; Pak, CY (1987). "Hypercalciuria and altered intestinal calcium absorption occurring independently of vitamin D in incomplete distal renal tubular acidosis". Metabolism: clinical and experimental. 36 (2): 176–9. doi:10.1016/0026-0495(87)90014-x. PMID 3807789.
- ↑ http://www.nasa.gov/exploration/humanresearch/analogs/research_info_analog-bedrest.html[]
- ↑ Zerwekh, JE; Odvina, CV; Wuermser, LA; Pak, CY (2007). "Reduction of renal stone risk by potassium-magnesium citrate during 5 weeks of bed rest". The Journal of Urology. 177 (6): 2179–84. doi:10.1016/j.juro.2007.01.156. PMID 17509313.
- ↑ http://microgravity.grc.nasa.gov/SOPO/ICHO/HRP/ExMC/IMM/[]
- ↑ Rambaut, Paul C.; Johnston, Richard S. (1979). "Prolonged weightlessness and calcium loss in man". Acta Astronautica. 6 (9): 1113–22. doi:10.1016/0094-5765(79)90059-6. PMID 11883480.
- 1 2 3 4 5 Risk of Renal Stone Formation (PDF). Human Research Program: Human Health Countermeasures Element (HRP-47060). NASA. March 2008. pp. 6–11.
- ↑ Whitson, PA; Pietrzyk, RA; Pak, CY; Cintrón, NM (1993). "Alterations in renal stone risk factors after space flight". The Journal of Urology. 150 (3): 803–7. PMID 8345588.
- ↑ Whitson, PA; Pietrzyk, RA; Pak, CY (1997). "Renal stone risk assessment during Space Shuttle flights". The Journal of Urology. 158 (6): 2305–10. doi:10.1016/s0022-5347(01)68240-5. PMID 9366381.
- ↑ Whitson, PA; Pietrzyk, RA; Sams, CF (1999). "Space flight and the risk of renal stones". Journal of gravitational physiology. 6 (1): P87–8. PMID 11543039.
- ↑ Whitson, PA; Pietrzyk, RA; Morukov, BV; Sams, CF (2001). "The risk of renal stone formation during and after long duration space flight". Nephron. 89 (3): 264–70. doi:10.1159/000046083. PMID 11598387.
- ↑ http://lsda.jsc.nasa.gov/scripts/experiment/exper.cfm?exp_index=902[]
- ↑ Whitson, PA; Pietrzyk, RA; Jones, JA; Nelman-Gonzalez, M; Hudson, EK; Sams, CF (2009). "Effect of potassium citrate therapy on the risk of renal stone formation during spaceflight" (PDF). The Journal of Urology. 182 (5): 2490–6. doi:10.1016/j.juro.2009.07.010. PMID 19765769.
External links
- NASA Human Research Wiki - ExMC Gap Report 4.13 Limited Capability to Diagnose and Treat a Renal Stone
- Renal Stone Risk During Space Flight: Assessment and Countermeasure Validation
- Twinkle, twinkle kidney stone: With a push you could be gone
- UW Researchers Develop Ultrasound Technology That Detects and Treats Kidney Stones in Space
- Ciftçioglu, N; Haddad, RS; Golden, DC; Morrison, DR; McKay, DS (2005). "A potential cause for kidney stone formation during space flights: Enhanced growth of nanobacteria in microgravity". Kidney International. 67 (2): 483–91. doi:10.1111/j.1523-1755.2005.67105.x. PMID 15673296.
![]() This article incorporates public domain material from the National Aeronautics and Space Administration document "Human Health and Performance Risks of Space Exploration Missions" (NASA SP-2009-3405).
This article incorporates public domain material from the National Aeronautics and Space Administration document "Human Health and Performance Risks of Space Exploration Missions" (NASA SP-2009-3405).