ZS-9
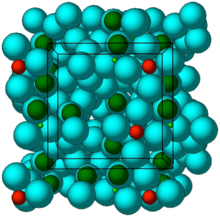 Crystal structure of ZS-9. Blue spheres = oxygen atoms, red spheres = zirconium atoms, green spheres = silicon atoms. | |
| Clinical data | |
|---|---|
| Routes of administration | Oral |
| ATC code | none |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | Not absorbed |
| Excretion | Stool |
| Identifiers | |
| |
| CAS Number | 242800-27-7 |
| UNII | D652ZWF066 |
| Chemical and physical data | |
| Formula | (2Na·H2O·3H4SiO4·H4ZrO6)n |
ZS-9 (sodium zirconium cyclosilicate) is a selective oral sorbent that traps potassium ions throughout the gastrointestinal tract. It is being developed by ZS Pharma and AstraZeneca for the treatment of hyperkalemia (elevated serum potassium levels).[1]
Background
Hyperkalemia occurs in 3 to 10% of hospitalized patients[2] but is often mild. Hyperkalemia can arise from impaired renal function, potassium-sparing diuretics and renin-angiotensin system blockers (e.g., ACE inhibitors, angiotensin receptor blockers, spironolactone) and diabetes mellitus.[2][3][4][5]
There is no universally accepted definition of what level of hyperkalemia is mild, moderate, or severe.[6] However, if hyperkalemia causes any ECG change it is considered a medical emergency[6] due to a risk of potentially fatal abnormal heart rhythms (arrhythmia) and is treated urgently.[6] serum potassium concentrations greater than 6.5 to 7.0 mmol/L in the absence of ECG changes are managed aggressively.[6]
Hyperkalemia, particularly if severe, is a marker for an increased risk of death.[2] However, there is disagreement regarding whether a modestly elevated serum potassium level directly causes significant problems. One viewpoint is that mild to moderate hyperkalemia is a secondary effect that denotes significant underlying medical problems.[2] Accordingly, these problems are both proximate and ultimate causes of death,[2] and adjustment of potassium may not be helpful. Alternatively, hyperkalemia may itself be an independent risk factor for cardiovascular mortality.[7]
Several approaches are used in the treatment of hyperkalemia.[6] In October 2015, the U.S. Food and Drug Administration (FDA) approved patiromer which works by binding free potassium ions in the gastrointestinal tract and releasing calcium ions for exchange. Previously, the only approved product was sodium polystyrene sulfonate (Kayexalate),[8] an organic ion-exchange resin that nonspecifically binds cations (e.g., calcium, potassium, magnesium) in the gastrointestinal tract. The effectiveness of sodium polystyrene sulfonate has been questioned: a study in healthy subjects showed that laxatives alone were almost as effective in increasing potassium secretion as laxatives plus Kayexalate.[9] In addition, use of sodium polystyrene sulfonate, particularly if formulated with high sorbitol content, is uncommonly but convincingly associated with colonic necrosis.[6][8][10][11]
Mechanism of action
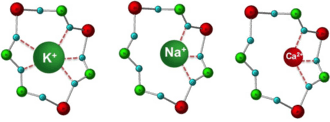
ZS-9 is a zirconium silicate. Zirconium silicates have been extensively used in medical and dental applications because of their proven safety.[12] 11 zirconium silicates were screened by an iterative optimization process. ZS-9 selectively captures potassium ions, presumably by mimicking the actions of physiologic potassium channels.[13] ZS-9 is an inorganic cation exchanger crystalline with a high capacity to entrap monovalent cations, specifically potassium and ammonium ions, in the GI tract. ZS-9 is not systemically absorbed; accordingly, the risk of systemic toxicity may be minimized.
Clinical studies
A phase 2 clinical trial in 90 patients with chronic kidney disease and mild-to-moderate hyperkalemia found a significantly greater reduction in serum potassium with ZS-9 than placebo. ZS-9 was well tolerated, with a single adverse event (mild constipation).[14]
A double-blind, phase 3 clinical trial in 753 patients with hyperkalemia and underlying chronic kidney disease, diabetes, congestive heart failure, and in patients on renin-angiotensin system blockers compared ZS-9 with placebo.[15] Patients were randomly assigned to receive either ZS-9 (1.25 g, 2.5 g, 5 g, or 10 g) or placebo 3 times daily for 48 hours (acute phase). Patients who achieved normokalemia (serum potassium of 3.5-4.9 mmol/L) were randomly assigned to receive ZS-9 or placebo once daily for 12 additional days (maintenance phase). At the end of the acute phase, serum potassium significantly decreased in the 2.5 g, 5 g, and 10 g ZS-9 groups. During the maintenance phase, once daily 5 g or 10 g ZS-9 maintained serum potassium at normal levels. Adverse events, including specifically gastrointestinal effects, were similar with either ZS-9 or placebo.[15]
A double-blind, phase 3 clinical trial in 258 patients with hyperkalemia and underlying chronic kidney disease, diabetes, congestive heart failure, and in patients on renin-angiotensin system blockers compared ZS-9 with placebo.[16] All patients received 10 g ZS-9 three times daily for 48 hours in the initial open-label phase. Patients who achieved normokalemia (serum potassium 3.5-5.0 mEq/L) were randomly assigned to receive either ZS-9 (5 g, 10 g, or 15 g) or placebo once daily for 28 days (double-blind phase). 98% of patients (n=237) achieved normokalemia during the open-label phase. During the double-blind phase, once daily 5 g, 10 g, and 15 g ZS-9 maintained serum potassium at normal levels in a significantly higher proportion of patients (80%, 90%, and 94%, respectively) than placebo (46%). Adverse events were generally similar with either ZS-9 or placebo. Hypokalemia occurred in more patients in the 10 g and 15 g ZS-9 groups (10% and 11%, respectively), versus none in the 5 g ZS-9 or placebo groups.[16]
Regulatory
In the United States, regulatory approval of ZS-9 was rejected by the Food and Drug Administration in May 2016 due to issues associated with manufacturing.[17]
See also
- Patiromer, another potassium binder
References
- ↑ "ZS-9. A selective potassium binder". ZS-Pharma.
- 1 2 3 4 5 Elliott, M. J.; Ronksley, P. E.; Clase, C. M.; Ahmed, S. B.; Hemmelgarn, B. R. (2010). "Management of patients with acute hyperkalemia". Canadian Medical Association Journal. 182 (15): 1631–5. doi:10.1503/cmaj.100461. PMC 2952010
 . PMID 20855477.
. PMID 20855477. - ↑ Stevens, M. S.; Dunlay, R. W. (2000). "Hyperkalemia in hospitalized patients". International Urology and Nephrology. 32 (2): 177–80. doi:10.1023/A:1007135517950. PMID 11229629.
- ↑ Tamirisa, K. P.; Aaronson, K. D.; Koelling, T. M. (2004). "Spironolactone-induced renal insufficiency and hyperkalemia in patients with heart failure". American Heart Journal. 148 (6): 971–8. doi:10.1016/j.ahj.2004.10.005. PMID 15632880.
- 1 2 3 4 5 6 Taal, M.W.; Chertow, G.M.; Marsden, P.A.; Skorecki, K.; Yu, A.S.L.; Brenner, B.M. (2012). Brenner and Rector's The Kidney (Chapter 17, page 672, 9th ed.). Elsevier. ISBN 978-1-4160-6193-9.
- ↑ Fang, J.; Madhavan, S.; Cohen, H.; Alderman, M. H. (2000). "Serum potassium and cardiovascular mortality". Journal of General Internal Medicine. 15 (12): 885–90. doi:10.1046/j.1525-1497.2000.91021.x. PMID 11119186.
- 1 2 Watson, M.; Abbott, K. C.; Yuan, C. M. (2010). "Damned if You Do, Damned if You Don't: Potassium Binding Resins in Hyperkalemia". Clinical Journal of the American Society of Nephrology. 5 (10): 1723–6. doi:10.2215/CJN.03700410. PMID 20798253.
- ↑ Emmett, M.; Hootkins, R. E.; Fine, K. D.; Santa Ana, C. A.; Porter, J. L.; Fordtran, J. S. (1995). "Effect of three laxatives and a cation exchange resin on fecal sodium and potassium excretion". Gastroenterology. 108 (3): 752–60. doi:10.1016/0016-5085(95)90448-4. PMID 7875477.
- ↑ Sterns, R. H.; Rojas, M.; Bernstein, P.; Chennupati, S. (2010). "Ion-Exchange Resins for the Treatment of Hyperkalemia: Are They Safe and Effective?". Journal of the American Society of Nephrology. 21 (5): 733–5. doi:10.1681/ASN.2010010079. PMID 20167700.
- ↑ Kamel, K. S.; Schreiber, M. (2012). "Asking the question again: Are cation exchange resins effective for the treatment of hyperkalemia?". Nephrology Dialysis Transplantation. 27 (12): 4294–7. doi:10.1093/ndt/gfs293. PMID 22989741.
- ↑ Denry I, Kelly JR. State of the art of zirconia for dental applications. Dental Materials. Volume 24, Issue 3, March 2008, Pages 299–307
- ↑ =Stavros, F (2014). "Characterization of Structure and Function of ZS-9, a K⁺ Selective Ion Trap". PLOS ONE. 9 (12): e114686. doi:10.1371/journal.pone.0114686. PMC 4273971. PMID 25531770.
- ↑ Ash SR, et al. "Safety and efficacy of ZS-9, a novel selective cation trap, for treatment of hyperkalemia in CKD patients." American Society of Nephrology 2013 conference, Late-Breaking Abstract.
- 1 2 Packham DK, et al. (2014). "Sodium zirconium cyclosilicate in hyperkalemia". New England Journal of Medicine. 372 (3): 222–31. doi:10.1056/NEJMoa1411487. PMID 25415807.
- 1 2 Kosiborod M, et al. (2014). "Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia". Journal of the American Medical Association. 312 (21): 2223–33. doi:10.1001/jama.2014.15688. PMID 25402495.
- ↑ Ben Adams (May 27, 2016). "AstraZeneca's $2.7B hyperkalemia drug ZS-9 rejected by FDA". FierceBiotech.