Duodenal cancer
| Duodenal cancer | |
|---|---|
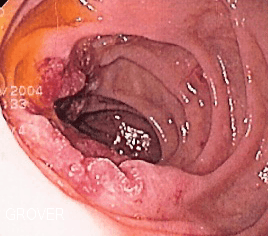 | |
| Endoscopic image of adenocarcinoma of duodenum seen in the post-bulbar duodenum | |
| Classification and external resources | |
| Specialty | oncology |
| ICD-10 | C17.0 |
| ICD-9-CM | 152.0 |
| MeSH | D004379 |
Duodenal cancer is a cancer in the beginning section of the small intestine. It is relatively rare compared to gastric cancer and colorectal cancer. Its histology is usually adenocarcinoma. Familial adenomatous polyposis (FAP), Gardner Syndrome, Lynch Syndrome, Muir-Torre syndrome, Celiac sprue, Puetz-Jeghers, Crohn's Disease and Juvenile Polyposis Syndrome are risk factors for developing this cancer.[1]
The duodenum is the first part of the small intestine. It is located between the stomach and the jejunum. After foods combine with stomach acid, they descend into the duodenum where they mix with bile from the gall bladder and digestive juices from the pancreas.
Treatment
Resection is sometimes a part of a treatment plan,[2] but duodenal cancer is difficult to remove surgically because of the area that it resides in—there are many blood vessels supplying the lower body. Chemotherapy is sometimes used to try to shrink the cancerous mass. Other times intestinal bypass surgery is tried to reroute the stomach to intestine connection around the blockage.
A 'Whipple' procedure is a type of surgery that is sometimes possible with this cancer. In this procedure, the duodenum, a portion of the Pancreas (the head), and the gall bladder are usually removed, the small intestine is brought up to the Pylorus (the valve at the bottom of the stomach) and the Liver and Pancreas digestive enzymes and bile are connected to the small intestine below the Pylorus.
The removal of part of the Pancreas often requires taking Pancreatic Enzyme supplements to aid digestion. These are available in the form of capsules by prescription.
It is not unusual for a patient having received a Whipple procedure to feel perfectly well, and to lead his/her normal life without difficulty.
It is important for the procedure to be performed by a surgeon with extensive experience having done and observed the procedure, as specific competence makes a big difference.
Some patients need to be fitted with tubes to either add nutrients (feeding tubes) or drainage tubes to remove excess processed food that can not pass the blockage.
Presentation
The cancerous mass tends to block food from getting to the small intestine. If food cannot get to the intestines, it will cause pain, acid reflux, and weight loss because the food cannot get to where it is supposed to be processed and absorbed by the body.
Patients with duodenal cancer may experience abdominal pain, weight loss, nausea, vomiting, and chronic GI bleeding.
References
- ↑ Kalogerinis PT, Poulos JE, Morfesis A, et al. (2010). "Duodenal carcinoma at the ligament of Treitz. A molecular and clinical perspective". BMC Gastroenterol. 10: 109. doi:10.1186/1471-230X-10-109. PMC 2949773
 . PMID 20849628.
. PMID 20849628. - ↑ Gold JS, Tang LH, Gönen M, Coit DG, Brennan MF, Allen PJ (November 2007). "Utility of a prognostic nomogram designed for gastric cancer in predicting outcome of patients with R0 resected duodenal adenocarcinoma". Annals of Surgical Oncology. 14 (11): 3159–67. doi:10.1245/s10434-007-9542-1. PMID 17680313.