Health in Uganda

As a developing country, health in Uganda lags behind many other countries but is at par with the countries in the World Health Organization's (WHO) Africa region. As of 2013, life expectancy at birth in Uganda was 58 years, lower than any other country in the East African Community except for Burundi.[1] As of 2015, the probability of a child dying before reaching age five was 5.5 percent (55 deaths for every 1,000 live births).[2] Total health expenditure as a percentage of GDP was 7.2 percent in 2014.[3]
Uganda was hit very hard by the outbreak of the HIV/AIDS epidemic in East Africa. In the early 1990s, 13 percent of Ugandan residents had HIV. This had fallen to 4.1 percent by the end of 2003, the most effective national response to AIDS of any African country (see AIDS in Africa). As at 2015, the HIV prevalence rate in the country was 7.2 percent.[4]
Uganda is home to the Uganda Virus Research Institute, considered one of the most advanced viral research facilities in East Africa and one of the three countries where randomised controlled trials for male circumcision were conducted to inform the WHO policy decision on voluntary medical circumcision.[5]
Health infrastructure
Uganda's health system is composed of health services delivered in the public sector, by private providers, and by traditional and complementary health practitioners. It also includes community-based health care and health promotion activities. The aim of Uganda’s health system is to deliver the national minimum health care package. Uganda runs a decentralized health system with national and district levels.[6]
Structure of Uganda's health system
Uganda’s health system is divided into national and district-based levels. At the national level are the national referral hospitals, regional referral hospitals, and semi-autonomous institutions including the Uganda Blood Transfusion Services, the National Medical Stores, the Uganda Public Health Laboratories and the Uganda National Health Research Organization (UNHRO).[6]
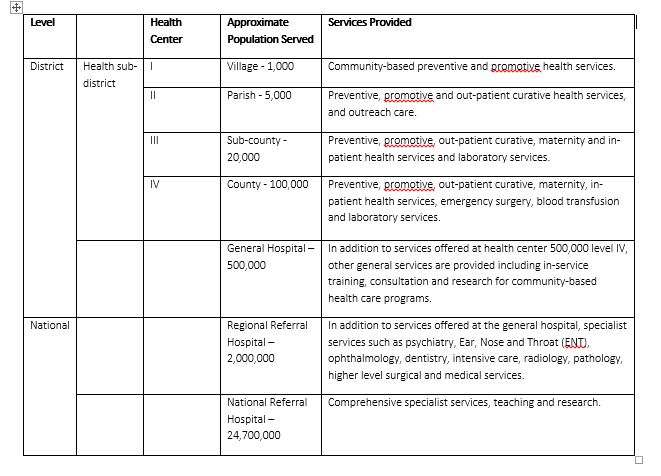
The lowest rung of the district-based health system consists of Village Health Teams (VHTs). These are volunteer community health workers who deliver predominantly health education, preventive services, and simple curative services in communities. They constitute level 1 health services. The next level is Health Center II, which is an out patient service run by a nurse. It is intended to serve 5,000 peoole. Next in level is Health Center III (HCIII) which serves 10,000 people and provides in addition to HC II services, in patient, simple diagnostic, and maternal health services. It is managed by a clinical officer. Above HC III is the Health Center IV, run by a medical doctor and providing surgical services in addition to all the services provided at HC III. HC IV is also intended to provide blood transfusion services and comprehensive emergency obstetric care.[7]
The table below summarizes the district-based health system.
Health system reforms
At the beginning of the 21st century, the government of Uganda began implementing a series of health sector reforms that were aimed at improving the poor health indicators prevailing at the time. A Sector-Wide Approach (SWAp) was introduced in 2001 to consolidate health financing.[8] Another demand side reform introduced in the same year was the abolition of user fees at public health facilities, which triggered a surge in outpatient attendances across the country.[9][10]
Decentralization of health services began in the mid-1990s alongside wider devolution of all public administration, and was sealed in 1998 with the definition of the health sub-district. Implementation of the health sub district concept extended into the early 2000s.[11]
To improve medicines management and availability, the government of Uganda made medicines available to private-not-for-profit (PNFP) providers. With decentralization of health services, a "pull" system was instituted in which district and health facility managers were granted autonomy to procure medicines they needed in the required quantities from the national medical stores, within pre-set financial earmarks. The result was better availability of medicines.[12]
Health system performance
A comprehensive review of Uganda’s Health System conducted in 2011 uncovered strengths and weaknesses of the health system, organized around the six technical building blocks of health system that were defined by the WHO. In summary the assessment found that whereas significant efforts are being implemented to qualitatively and quantitatively improve health in Uganda, more needs to be done to focus on the poor, improve engagement of the private-for-profit sector, enhance efficiency, strengthen stakeholder coordination, improve service quality, and stimulate consumer-based advocacy for better health. The Ministry of Health (MOH) also conducts annual health sector performance appraisals that assess health system performance and monitor progress in delivery of the UNMHCP.[12]
Health workforce
A Human Resources for Health Policy is in place to guide recruitment, deployment, and retention of health staff. In spite of this, shortages of health workers persist. There is one doctor for every 7,272 Ugandans. The related statistic is 1:36,810 for nurse/midwifery professionals. The shortages are worse in rural areas where 80 percent of the population resides, as 70 percent of all doctors are practicing in urban areas.[13]
Health financing
Total public and private health expenditure per capita was US$59 in 2013.[14] Public financing for health was 4.3 percent of GDP in 2013,[15] well below the target of 15 percent set in the 2001 Abuja Declaration.[16]
Health information systems
Uganda has transitioned to a computerized web-based system in 2013 (DHIS 2). This is expected to improve use of real-time data for planning and budgeting.[17]
Service delivery
According to the Uganda National Household Survey 2012/2013, the majority of those who sought for health care first visited a private hospital/clinic (37 percent) or a government health centre (35 percent). Twenty two percent of the urban population used Government health centers, while that proportion rose to 39 percent in the rural areas. Thirty five percent of government health centers visited by persons who fell sick were within a radius of 5 kilometres (3 mi) from the population.[18]
Medical products, vaccines, and technologies
Management of essential medicines and supplies is a weak point of Uganda’s health system. Drug shortages are prevalent.[19]
Governance and stewardship
All relevant policies and regulations are in place. The MOH is currently implementing the HSSIP, which is the third iteration of health sector strategies. The MOH coordinates stakeholders and is responsible for planning, budgeting, policy formulation, and regulation.[11]
The health sector at the district and sub-district level is governed by the district health management team (DHMT). The DHMT is led by the district health officer (DHO) and consists of managers of various health departments in the district. The heads of health sub-districts (HC IV managers) are included on the DHMT. The DHMT oversees implementation of health services in the district, ensuring coherence with national policies. A Health Unit Management Committee (HUMC) composed of health staff, civil society, and community leaders is charged with linking health facility governance with community needs.[11]
Reproductive health
Reproductive health (RH) is a state of complete physical, mental, and social well-being in all matters relating to the reproductive system and to its functions and processes. It implies that people have the capability to reproduce and the freedom to decide if, when, and how often to do so. Implicit in this is the right of men and women to be informed and to have access to safe, effective, affordable, and acceptable methods of family planning of their choice, as well as other methods of their choice for regulation of fertility, which are not against the law, and the right of access to health-care services that will enable women to go safely through pregnancy and childbirth. RH care also includes sexual health, the purpose of which is the enhancement of life and personal relations.[20]
Fertility rate and family planning
Uganda has the second-highest fertility rate in the East African Community, behind only Burundi. According to 2014 data, a Ugandan woman, on average, gives birth to 5.8 children during her lifetime compared to 7.0 in 1960 and 6.8 in 2001.[21] The age-specific fertility rates indicate that fertility peaks when women are aged between 20 and 24 years and then declines slowly until age 34. According to 2011 data, the fertility rate in urban areas (3.8 per woman), significantly lower than in rural areas (6.7 per woman ).[22]
Thirty percent of married Ugandan women are using some method of contraception, with 26 percent using modern contraceptive methods (MCM), such as female and male sterilization, pill, intrauterine device, injectables, implants, male condom, diaphragm, and the lactational amenorrhea method. MCM were used by only 8 percent of married Ugandan women in 1995.[22] There is a gap between the demand for contraception and the amount of contraception being made available. Several organisations are providing health education and contraceptive services.[23]
Antenatal care, facility deliveries, and postnatal care
Antenatal care (ANC) coverage in Uganda in 2011 was almost universal with above 95 percent of women attending at least one visit. However, only 48 percent of women attended the recommended four visits. The two proportions have remained stagnant since 2006. Deliveries in health facilities account for about 57 percent of all deliveries, far below the number of women who attend at least one ANC visit. That percentage had risen from 41 percent over a five-year period.[22]
Only one-third of women received postnatal care (PCN) in the first two days after delivery. In 2011, only two percent of mothers received a PNC check up in the first hour for all births in two years before the 2011 Uganda Demographic Household Survey.[22]
Table: Uganda Trends in Selected SRH indicators[22]
| Indicator | 1980 | 1995 | 2000 | 2006 | 2011 |
|---|---|---|---|---|---|
| Births attended by skilled health staff (% of total) | 38 | 39 | 42 | 58 | |
| Maternal Mortality Ratio | 435 | 561 | 505 | 435 | 438 |
| Contraceptive Prevalence rate | 19 | 24 | 30 | ||
| Unmet Need for FP | 35 | 41 | 34 | ||
| Total fertility rate | 7.1 | 7.1 | 6.9 | 6.7 | 6.2 |
| HIV Prevalence (% of Adult Population) | 10.2 | 7.3 | 6.7 | 7.3 | |
| Percentage of men (15-59) circumcised | 25 | 27 | |||
Sexual health
Sexual health in Uganda is affected by the high prevalence of HIV with a generalized epidemic and several STIs, the poor health seeking behaviours regarding STIs, violence and some practices such as FGM that affect female sexuality in isolated communities north east parts of the country. As at 2015, Uganda's national HIV prevalence rate was 7.2 among adults aged 15 – 59 years. This has increased from 6.7 in 2005.[4] Prevention has now included a new measure of male circumcision, although sexual behaviors among circumcised men need more understanding.[24]
Men's health
There are issues that affect men including violence, sexually transmitted diseases, prostate cancers, infertility, HIV specifically, other NCDs that affect sexual performance. The latest intervention that could improve men's sexual health is male circumcision. This could also have benefits on the women's health in the long run with reduced HIV prevalence among men if population interventions are successful.[25]
Maternal and child health
.jpg)
The 2010 maternal mortality rate per 100,000 births for Uganda is 430. This is compared with 352.3 in 2008 and 571 in 1990. The under-five mortality rate, per 1,000 births is 130 and the neonatal mortality as a percentage of under-fives' mortality is 24.[26] In Uganda, the number of midwives per 1,000 live births is 7 and 1 in 35 is the lifetime risk of death for pregnant women.[26]
Maternal health

The World Health Organization (WHO) defines maternal health as the health of women during pregnancy, childbirth and the postpartum period.[27] According to estimates from UNICEF, Uganda’s maternal mortality ratio, the annual number of deaths of women from pregnancy-related causes per 100,000 live births,[28] stood at 440 in the 2008 - 2012 time frame.[29]
With the 2015 target for maternal mortality ratio at 131 per 100,000 births and proportion of births attended by skilled health personnel set at 100%,[30] Uganda has a long battle in reaching its intended goals. Moreover, the methodology used and the sample sizes implemented by the Uganda Demographic Health Survey (UDHS) do not allow for precise estimates of maternal mortality.[30]
In rural areas, conceiving pregnant women seek the help of traditional birth attendants (TBAs) due to difficulty in accessing formal health services and also high transportation or treatment costs. TBAs are trusted as they embody the cultural and social life of the community. However, the TBAs’ lack of knowledge and training and the use of traditional practices have led to risky medical procedures resulting in high maternal mortality. High maternal mortality rates persist in Uganda due to an overall low use of contraceptives, limited capacity of health facilities to manage abortion/miscarriage complications and prevalence of HIV/AIDS among pregnant women. Despite malaria being one of the leading causes of morbidity in pregnant women, prevention and prophylaxis services are not well established.[31]
Almost all women in developing countries have at least four antenatal care visits, are attended to by a skilled health worker during childbirth and receive postpartum care. In contrast, only 47% of Ugandan women receive the recommended four antenatal care visits and only 42% [29] of births are attended by skilled health personnel. Among the poorest 20% of the population, the share of births attended by skill health personnel was 29% in 2005/2006 as compared to 77% among the wealthiest 20% of the population.[30] The case of Jennifer Anguko, a popular elected official who bled slowly to death in the maternity ward in a major hospital, aptly exemplifies the poor state of maternal health care that is provided to women, even in major urban healthcare facilities.[32]
Despite the national policy of promoting maternal health through promoting informed choice, service accessibility and improved quality of care through the national Safe Motherhood Programme (SMP), it remains a challenge to the Ugandan government as to how it would achieve its 2015 Millennium Development Goals of reducing maternal mortality rates and 100% births attended to by skilled health personnel. In order to achieve future economic growth, it is vital that the population remains healthy.[33]
Gender based violence
Domestic Violence (DV) is a key issue in reproductive health and rights and most of the DV is gender-based.[34] Domestic violence is prevalent in Uganda especially among women. Physical violence is the most prevalent with one quarter of women reporting it. Intimate partner violence is the most common form of violence in Uganda that could affect reproductive health right. more than 60% of women who were ever married report having experienced emotional, physical, or sexual violence from a spouse and several of them have experienced physical injuries as a result.[35]
In 2011, about 2% of women reported to have undergone FGM, a practice that is dying away in the areas where it was more practiced.[22]
Health in the Northern Region
Northern Uganda is one of the four major administrative regions in Uganda. The region was devastated by a protracted civil war between the government of Uganda and the Lords Resistance Army as well as the cattle rustling conflict that lasted for 20 years.[36][37]
Since the war ended in 2006, the IDP camps have been destroyed and people have resettled back to their former homesteads. The region, however, still has many health challenges, such as poor health care infrastructure and inadequate staffing at all levels;[38] lack of access to the national electricity grid;[39] an inability to attract and retain qualified staff; frequent stock outs in the hospitals and health facilities; poverty; emerging and re-emerging diseases such as Ebola, nodding syndrome, onchocerciasis, and tuberculosis;[40] malaria epidemics; reintegration of former abducted child soldiers who returned home;[41] lack of safe drinking water as most boreholes were destroyed during the war; the HIV/AIDS epidemic;[42] poor education standards with high failure rates in primary and secondary school national examinations;[43][44] and poverty.[45]
Health indicators
According to the 2015 Uganda Bureau of Statistics (UBOS) report:[46]
- The region has one of the highest HIV prevalence rates of 8 percent in the country, second only to Kampala.
- The region leads in poverty with 80 percent of households living below poverty line compared to only 20 percent of the country in general living in poverty. The region has the lowest per capita house hold expenditure of UGX:21,000 compared to UGX:30,000 of the general population. Up to 26 percent of people are chronically poor
- The region leads in illiteracy with only 60 percent of the population aged 10 years and above being literate compared to 71 percent of the general country population.
- Most districts in the region lack clean piped water supply with the exception of a few town centers like Gulu, Lira, Arua, and Soroti. The pit latrine coverage ranges from 4 to 84 percent in some districts, the worst in the country.
- The region has the lowest numbers of health facilities compared to other regions of the country. Of the total 5,229 health facilities in Uganda (2,867 operated by the government, 874 operated by non-governmental organizations (NGOs), and 1,488 private facilities), there are only 788 health facilities in the Northern Region (664 operated by government, 122 operated by NGOs, and 2 private facilities). Health facility deliveries range from 7 percent in Amudat, to 81 percent in Gulu.[46]
- The region has the highest total fertility rate of 7.9 children per woman compared to the nationwide 6.1 rate.[22]
- The Karamoja sub-region has high maternal mortality ratios.[47] According to the 2001 Uganda Demographic and Health Survey, the Northern Region was the worst in infant child mortality indicators (under age 5 mortality: 178 deaths per 1000 live births) (under age 1 mortality: 105 deaths per 1000 live births) (neonatal mortality: 42 deaths within the first month of life per 1000 live births).[30] For purposes of the 2011 Uganda Demographic and Health Survey, the Northern Region was subdivided into West Nile, North, and Karamoja, with the other three regions having seven subdivisions, for a total of ten subdivisions nationwide. Karamoja's under age 5 mortality rate (153 deaths per 1000 live births) was the worst in the country, with West Nile's rate (125) the third worst and the North's rate (105) the fourth best. West Nile's under age 1 mortality rate (88) was the worst in the country, with Karamoja's rate (87) the second worst and the North's rate (66) the fifth best. West Nile's under one month mortality rate (38) was the second worst in the country, with the North's rate (31) tied for fourth worst and Karamoja's rate (29) being the fourth best.[30]
- Nodding syndrome hit the region during the early to mid-2000s only be come to the knowledge of the international community in 2009, when the World Health Organization and the US Centers for Disease Control first went to investigate it.[48] The disease affected children aged 5–15 years, mainly in the Acholi sub-region and a few in the Lango sub-region.[49] Over 3,000 confirmed cases were documented and are undergoing treatment in various treatment centers across the region, with Uganda having the highest number of cases in the world.[50] The disease has profound health effects on children, families, and communities.[51] The children who were previously healthy and growing well are observed by the parents to nod mainly at meal times initially, progressing to head nod when it is cold, etc. These children eventually develop various forms of epileptic seizures as well as disabilities such as severe malnutrition, burns, contractures, severe kyphosis, cognitive impairment, and wandering away from homes.[52] Since the interventions began in 2012, there have been no new cases reported in the region. The exact cause of this disease has not been found although there is strong association with oncocerchiasis. Communities believe their children could have been exposed to chemicals during the war, particularly when they were displaced into IDPs camps because they observed that their children became sick only when in camps and not outside the camps.[53]
| ! Sub County | Nodding S | Nodding S | Epilepsy | Epilepsy |
|---|---|---|---|---|
| Male | Fenale | Male | Female | |
| Awere | 230 | 188 | 231 | 198 |
| Atanga | 144 | 129 | 95 | 84 |
| Lapul | 34 | 32 | 23 | 22 |
| Agagura | 119 | 108 | 70 | 64 |
| Laguti | 172 | 164 | 115 | 110 |
| Acholi Bur | 03 | 04 | 18 | 23 |
| Puranga | 13 | 12 | 148 | 146 |
| Pader | 13 | 11 | 21 | 16 |
| Total | 728 | 648 | 721 | 663 |
See also
References
- ↑ The World Bank (2013). "Life expectancy at birth, total (years)". Washington, DC: The World Bank. Retrieved 16 October 2016.
- ↑ The World Bank (2015). "Mortality rate, under-5 (per 1,000 live births)". Washington, DC: The World Bank. Retrieved 16 October 2016.
- ↑ The World Bank (2015). "Health expenditure, total (% of GDP)". Washington, DC: The World Bank. Retrieved 16 October 2016.
- 1 2 UNAIDS (2016). "Global information and advice on HIV & AIDS: HIV and AIDS in Uganda (2015)". Geneva: Avert.org Quoting UNAIDS Gap Report 2016. Retrieved 16 October 2016.
- ↑ WHO (July 2012). "Voluntary medical male circumcision for HIV prevention". Geneva: World Health Organisation (WHO). Retrieved 16 October 2016.
- 1 2 Stephen Mallinga. "The Second National Health Policy: Promoting People's Health to Enhance Socio-Economic Development", Uganda Ministry of Health, July 2010" (PDF). Kampala: World Health Organization (WHO) Quoting Ministry of Health (Uganda).
- ↑ MHU (2000). "Uganda Ministry of Health: Health Sector Strategic Plan 2000/01 – 2004/05" (PDF). Kampala: World Bank Quoting Ministry of Health (Uganda) (MHU). Retrieved 16 October 2016.
- ↑ Jeppsson A (December 2002). "SWAp dynamics in a decentralized context: experiences from Uganda". Social Science and Medicine. 55 (11): 2053–2060. PMID 12406470.
- ↑ Mylene Lagarde; Natasha Palmer (2008). "The impact of user fees on health service utilization in low- and middle-income countries: how strong is the evidence?". Bulletin of the World Health Organization. Geneva. 86 (11). Retrieved 16 October 2016.
- ↑ Ke Xu; David B Evans; Patrick Kadama; Juliet Nabyonga; Peter Ogwang Ogwal; Ana Mylena Aguilar (2005). "The elimination of user fees in Uganda: Impact on utilization and catastrophic health expenditures" (PDF). Geneva: World Health Organization. Retrieved 16 October 2016.
- 1 2 3 Tashobya C.; Nabyonga J.; Murindwa G.; Kyabaggu J.; Rutebemberwa E. (1 January 2006). "Meeting the challenges of decentralised health service delivery in Uganda as a component of broader health sector reforms". London: Department for International Development. Retrieved 17 October 2016.
- 1 2 Scott Stewart (2012). "Uganda Health System Assessment System Assessment 2011" (PDF). Washington, DC: United States Agency for International Development. Retrieved 16 October 2016.
- ↑ Africa Health Workforce Observatory (2009). "Human Resources for Health Country Profile, Uganda Members Document". Geneva: World Health Organisation. Retrieved 16 October 2016.
- ↑ The World Bank. "Health expenditure per capita (current US$)". Retrieved 28 February 2016.
- ↑ The World Bank. "Health expenditure, public (% of GDP)". Retrieved 28 February 2016.
- ↑ "The Abuja Declaration: Ten Years On", World Health Organization, 2011, accessed 28 February 2016
- ↑ The Republic of Uganda, Ministry of Health. Annual Health Sector Performance Report Financial Year 2012 / 2013. Kampala, Uganda. 2013
- ↑ "Uganda National Household Survey 2012/2013" (PDF). Kampala: Uganda Bureau of Statistics (UBOS). May 2014. Retrieved 16 October 2016.
- ↑ Athumani, Halima (7 August 2012). "NMS: Hospitals to Blame for Drug Shortages". Kampala: Uganda Radio Network. Retrieved 17 October 2016.
- ↑ WHO (17 October 2016). "Reproductive Health". Geneva: World Health Organisation (WHO). Retrieved 17 October 2016.
- ↑ The World Bank (2015). "Fertility rate, total (births per woman)". The World Bank. Retrieved 17 October 2016.
- 1 2 3 4 5 6 7 UBOS & ICFI (March 2012). "Uganda Demographic and Health Survey 2011" (PDF). Kampala & Calverton, Maryland, USA: Uganda Bureau of Statistics (UBOS) and ICF International Inc. (ICFI). Retrieved 17 October 2016.
- ↑ Nalwadda, Gorrette; Mirembe, Florence; Byamugisha, Josephat; Faxelid, Elisabeth (2010). "Persistent high fertility in Uganda: young people recount obstacles and enabling factors to use of contraceptives" (PDF). BMC Public Health. 10 (30). doi:10.1186/1471-2458-10-530. Retrieved 17 October 2016.
- ↑ Kibira, Simon Peter; Nansubuga, Elizabeth; Tumwesigye, Nazarius; Atuyambe, Lynn; Makumbi, Fredrick (2014). "Differences in risky sexual behaviors and HIV prevalence of circumcised and uncircumcised men in Uganda: evidence from a 2011 cross-sectional national survey" (PDF). Reproductive Health. 11 (25). doi:10.1186/1742-4755-11-25. Retrieved 3 September 2014.
- ↑ WHO (17 October 2016). "HIV/AIDS: Male circumcision for HIV prevention". Geneva: World Health Organization (WHO). Retrieved 17 October 2016.
- 1 2 UNFPA (August 2014). "The State of the World's Midwifery 2014: A Universal Pathway. A Woman's Right to Health". New York City: United Nations Population Fund (UNFPA). Retrieved 16 October 2016.
- ↑ WHO (17 October 2016). "World Health Organization: Maternal Health". World Health Organization (WHO).
- ↑ UNICEF (17 October 2016). "Women: Definitions of the indicators". Copenhagen: United Nations Children's Fund (UNICEF). Retrieved 17 October 2016.
- 1 2 UNICEF (17 October 2016). "Uganda Health Statistics". Copenhagen: United Nations Children's Fund (UNICEF). Retrieved 17 October 2016.
- 1 2 3 4 5 UNESCO (2014). "Millennium Development Goals Report for Uganda 2013" (PDF). Paris, France: United Nations Educational, Scientific and Cultural Organization (UNESCO). Retrieved 17 October 2016.
- ↑ Mugisa, Anne (10 April 2013). "Maternal mortality rate rises". New Vision. Kampala. Retrieved 17 October 2016.
- ↑ Dugger, Celia (29 July 2011). "Promising Care: Maternal Deaths Focus Harsh Light on Uganda". The New York Times. New York City. Retrieved 17 October 2016.
- ↑ The World Bank (23 October 2012). "Uganda Makes Progress on Maternal Health, But Serious Challenges Remain". Washington, DC: The World Bank. Retrieved 17 October 2016.
- ↑ WHO (17 October 2016). "Health topics: Violence against women". Geneva: World Health Organisation (WHO). Retrieved 17 October 2016.
- ↑ Richard Kavuma (8 March 2013). "International women's day: a voice from Mawokota County North, Uganda". The Guardian. London. Retrieved 17 October 2016.
- ↑ United Nations (2008). "Ten Stories the World Should Hear Moe About - Northern Uganda: Major Steps Towards Peace In A Decades-Old Conflict". New York City: United Nations. Retrieved 17 October 2016.
- ↑ Wegner, Patrick (9 April 2012). "A Genocide in Northern Uganda? – The 'Protected Camps' Policy of 1999 to 2006". Justiceinconflict.org. Retrieved 17 October 2016.
- ↑ Meredith McCormac, and Judy A. Benjamin PhD (October 2008). "Education and Fragility in Northern Uganda" (PDF). Washington, DC, United States of America: American Institutes for Research. Retrieved 17 October 2016.
- ↑ Brookings Institution (September 2007). "Peace, Recovery And Development Plan for Northern Uganda (PRDP)" (PDF). Washington, DC, USA: Brookings Institution. Retrieved 17 October 2016.
- ↑ Accorsi S., Fabiani M., Nattabi B., Corrado B., Iriso R., Ayella E. O., Pido B., Onek P. A., Ogwang M., Declich S. The disease profile of poverty: morbidity and mortality in northern Uganda in the context of war, population displacement and HIV/AIDS. Trans R Soc Trop Med Hyg. 2005 Mar;99(3):226-33
- ↑ BCFC (2007). "Resettlement of War-Affected Communities in Northern Uganda and the Longitudinal Folow-Up of the Reintegration Process of Former Child Soldiers". Ghent: Belgian Centre for Children in Vulnerable Situations (BCFC). Retrieved 17 October 2016.
- ↑ Associazione Volontari per il Servizio Internazionale (15 September 2004). "HIV seroprevalence in northern Uganda: The complex relationship between AIDS and conflict". Geneva: ReliefWeb. Retrieved 17 October 2016.
- ↑ Mwesigwa, Alon (23 April 2015). "Uganda's success in universal primary education falling apart". The Guardian. London. Retrieved 17 October 2016.
- ↑ Baguma, Raymond (23 January 2009). "Uganda: PLE - Bugisu, Mpigi, Kiboga, Amuru, Gulu Performed Worst". New Vision via AllAfrica.com. Kampala. Retrieved 17 October 2016.
- ↑ IFAD (2013). "Rural Poverty in Uganda". Rome, Italy: Ruralpovertyportal.org (RPPO) Quoting International Fund for Agricultural Development (IFAD). Retrieved 17 October 2016.
- 1 2 UBOS (October 2015). "Uganda Bureau of Statistics: 2015 Statistical Abstract" (PDF). Kampala: Uganda Bureau of Statistics (UBOS). Retrieved 17 October 2016.
- ↑ Anguyo, Innocent (27 March 2015). "Korea pledges USh25 billion to reduce maternal mortality". New Vision. Kampala. Retrieved 17 October 2016.
- ↑ WHO. "International Scientific Meeting on Nodding Syndrome, Kampala, Uganda, 30 July – 1 August 2012" (PDF). Geneva: World Health Organization (WHO). Retrieved 17 October 2016.
- ↑ Idro R, Musubire K A, Byamah Mutamba B, Namusoke H, Muron J, Abbo C, Oriyabuzu R, Ssekyewa J, Okot C, Mwaka D, Ssebadduka P, Makumbi I, Opar B, Aceng J R and Mbonye A K (2 June 2013). "Proposed guidelines for the management of nodding syndrome" (PDF). African Health Sciences. Retrieved 17 October 2016.
- ↑ Nakiyimba, Gloria (16 March 2012). "Northern Uganda has highest number of nodding syndrome cases". Paris, France: Radio France Internationale (RFI). Retrieved 17 October 2016.
- ↑ Dowell, Scott F.; Sejvar, James J.; Riek, Lul; Vandemaele, Katelijn A.H.; Lamunu, Margaret; Kuesel, Annette C.; Schmutzhard, Erich; Matuja, William; Bunga, Sudhir; Foltz, Jennifer; Nutman, Thomas B.; Winkler, Andrea S.; Mbonye, Anthony K. (2013). "Nodding Syndrome". Emerging Infectious Diseases. 19 (9): 1374–84. doi:10.3201/eid1909.130401. PMC 3810928
 . PMID 23965548.
. PMID 23965548. - ↑ Scott F. Dowell, James J. Sejvar, Lul Riek, Katelijn A.H. Vandemaele, Margaret Lamunu, Annette C. Kuesel, Erich Schmutzhard, William Matuja, Sudhir Bunga, Jennifer Foltz, Thomas B. Nutman, Andrea S. Winkler, and Anthony K. Mbonye (19 September 2013). "Nodding Syndrome". Emerging Infectious Diseases Journal. Atlanta. 19–9. Retrieved 17 October 2016.
- ↑ Mutamba, B; Abbo, C; Muron, J; Idro, R; Mwaka, AD (2013). "Stereotypes on Nodding syndrome: responses of health workers in the affected region of northern Uganda". African Health Sciences. 13 (4): 986–91. doi:10.4314/ahs.v13i4.18. PMC 4056485. PMID 24940322.
Notes
- UBOS and ICF International. Uganda Demographic and Health Survey 2011. Kampala, Uganda and Calverton, Maryland: Uganda Bureau of Statistics (UBOS) and ICF International Inc., 2012
- Uganda Bureau of Statistics (UBOS) and Macro International Inc. Uganda Demographic and Health Survey 2006. Calverton, Maryland, USA: UBOS and Macro International Inc: , 2007
- MOH and ICF International. Uganda AIDS Indicator Survey 2011. Kampala, Uganda and Calverton Maryland, USA: Ministry of Health and ICF International, 2012
- MOH and ORC Macro. Uganda HIV/AIDS Sero-behavioural Survey 2004-2005. Calverton, Maryland, USA: Ministry of Health and ORC Macro, 2006.
- Government of Uganda MOH. Safe Male Circumcision Policy. In: Ministry of Health, editor. Kampala 2010
- Population Reference Bureau. 2014 World Population Data sheet. Washington DC, USA: PRB; 2014 [www.prb.org]
- Population Reference Bureau. 2012 World Population Data sheet. Washington DC, USA: PRB; 2012 [www.prb.org]
- Population Reference Bureau. 2013 World Population Data sheet. Washington DC, USA: PRB; 2013 [www.prb.org]
External links
- The State of the World's Midwifery - Uganda Country Profile
- Film on Gideon Byamugisha and his fight against HIV stigma in Uganda
Uganda articles | |||||||
|---|---|---|---|---|---|---|---|
| History |  | ||||||
| Geography | |||||||
| Politics | |||||||
| Economy | |||||||
| Society |
| ||||||
| |||||||