Baker's cyst
| Baker's cyst or popliteal cyst | |
|---|---|
|
Schematic drawing of a Baker's cyst | |
| Classification and external resources | |
| Specialty | rheumatology |
| ICD-10 | M71.2 |
| ICD-9-CM | 727.51 |
| DiseasesDB | 1224 |
| MedlinePlus | 001222 |
| eMedicine | radio/72 |
| Patient UK | Baker's cyst |
| MeSH | D011151 |

A Baker's cyst, also known as a popliteal cyst, is a benign swelling of the semimembranosus or more rarely some other synovial bursa found behind the knee joint. It is named after the surgeon who first described it, William Morrant Baker (1838–1896).[1] It is not a "true" cyst, as an open communication with the synovial sac is often maintained.
Cause
In adults, Baker's cysts usually arise from almost any form of knee arthritis (e.g., rheumatoid arthritis) or cartilage (particularly a meniscus) tear. Baker's cysts in children do not point to underlying joint disease. Baker's cysts arise between the tendons of the medial head of the gastrocnemius and the semimembranosus muscles. They are posterior to the medial femoral condyle.
The synovial sac of the knee joint can, under certain circumstances, produce a posterior bulge, into the popliteal space, the space behind the knee. When this bulge becomes large enough, it becomes palpable and cystic. Most Baker's cysts maintain this direct communication with the synovial cavity of the knee, but sometimes, the new cyst pinches off. A Baker's cyst can rupture and produce acute pain behind the knee and in the calf and swelling of the calf muscles.
Diagnosis
Diagnosis is by examination. A Baker's cyst is easier to see from behind with the patient standing with knees fully extended. It is most easily palpated (felt) with the knee partially flexed. Diagnosis is confirmed by ultrasonography, although if needed and there is no suspicion of a popliteal artery aneurysm then aspiration of synovial fluid from the cyst may be undertaken with care. An MRI image can reveal presence of a Baker's cyst.
An infrequent but potentially life-threatening complication, which may need to be excluded by blood tests and ultrasonography, is a deep vein thrombosis (DVT). Quick assessment of the possibility of DVT may be required where a Baker's cyst has compressed vascular structures, causing leg edema, as this sets up conditions for a DVT to develop.
A burst cyst commonly causes calf pain, swelling and redness that may mimic thrombophlebitis.

Treatment
Baker's cysts usually require no treatment unless they are symptomatic. It is very rare that the symptoms are actually coming from the cyst. In most cases, there is another disorder in the knee (arthritis, meniscal (cartilage) tear, etc.) that is causing the problem. Initial treatment should be directed at correcting the source of the increased fluid production. Often rest and leg elevation are all that is needed. If necessary, the cyst can be aspirated to reduce its size, then injected with a corticosteroid to reduce inflammation. Surgical excision is reserved for cysts that cause a great amount of discomfort to the patient. A ruptured cyst is treated with rest, leg elevation, and injection of a corticosteroid into the knee. Recently, prolotherapy has shown encouraging results as an effective way to treat Baker's cysts and other types of musculoskeletal conditions.[2][3][4]
Baker's cysts in children, unlike in older people, nearly always disappear with time, and rarely require excision.
Ice pack therapy may sometimes be an effective way of controlling the pain related to Baker's cyst. Heat is also commonly used. A knee brace can offer support giving the feel of stability in the joint.
Rest and specific exercise
Many activities can put strain on the knee, and cause pain in the case of Baker's cyst. Avoiding activities such as squatting, kneeling, heavy lifting, climbing, and even running can help prevent pain. Despite this, some exercises can help relieve pain, and a physiotherapist may instruct on stretching and strengthening the quadriceps and/or the patellar ligament.
Gallery
-

Baker's cyst (popliteal cyst) is located behind the knee and is a swelling of the popliteal bursa. In this image, the Baker's cyst is the yellowish bulbous tissue which was identified during routine dissection.
-

Baker's cyst on axial MRI with communicating channel between the semimebranosus muscle and the medial head of the gastrocnemius muscle.
-

Baker's cyst on MRI, sagittal image
-
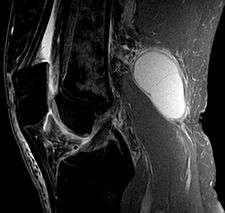
Baker's cyst on MRI, sagittal image
References
Notes
- ↑ "William Morrant Baker". Who Named It.
- ↑ "Alternative treatments. Dealing with chronic pain". Mayo Clinic health letter (English ed.). 23 (4): 1–3. 2005. PMID 15864836.
- ↑ Darrow, March (2004). Prolotherapy: Living Pain Free. Protex Press. ISBN 0-9714503-2-3.
- ↑ "Treatment of Baker's Cyst". North Yorkshire Orthopaedic Specialists. Retrieved 15 February 2013.
Bibliography
- Hellmann, DB (2005). "Chapter 20: Arthritis & Musculoskeletal Disorders". In Tierney LM, Jr.; McPhee SJ; Papadakis MA. Current Medical Diagnosis & Treatment (44th ed.). Philadelphia, PA: F. A. Davis Company. ISBN 0-07-145323-7.
- Joint Healing.com-Baker's Cyst
External links
| Wikimedia Commons has media related to Baker's cyst. |