Carcinoma in situ
| Carcinoma in situ | |
|---|---|
 | |
| Classification and external resources | |
| ICD-O | M8010/2 |
Carcinoma in situ (CIS), also known as in situ neoplasm, is a group of abnormal cells.[1][2] While they are a form of neoplasm[3] there is disagreement over whether CIS should be classified as cancer. This controversy also depends on the exact CIS in question (i.e. cervical, skin, breast). Some authors do not classify them as cancer, however, recognizing that they can potentially become cancer.[1] Others classify certain types as a non-invasive form of cancer.[4][5] The term "pre-cancer" has also been used.
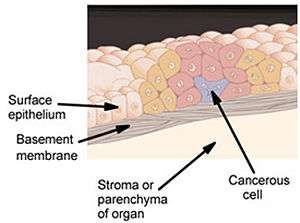
These abnormal cells grow in their normal place, thus "in situ" (from Latin for "in its place"). For example, carcinoma in situ of the skin, also called Bowen's disease, is the accumulation of dysplastic epidermal cells within the epidermis only, that has failed to penetrate into the deeper dermis. For this reason, CIS will usually not form a tumor. Rather, the lesion is flat (in the skin, cervix, etc.) or follows the existing architecture of the organ (in the breast, lung, etc.). Exceptions include CIS of the colon (polyps), the bladder (preinvasive papillary cancer), or the breast (ductal carcinoma ''in situ'' or lobular carcinoma in situ).
Many forms of CIS have a high probability of progression into cancer,[6] and therefore removal may be recommended; however, progression of CIS is known to be highly variable and not all CIS becomes invasive cancer.
In the TNM classification, carcinoma in situ is reported as TisN0M0 (stage 0).[7]
Terminology
These terms are related since they represent the steps of the progression toward cancer:
- Dysplasia is the earliest form of precancerous lesion recognizable in a biopsy. Dysplasia can be low-grade or high-grade. High-grade dysplasia may also be referred to as carcinoma in situ.
- Invasive carcinoma, usually simply called cancer, has the potential to invade and spread to surrounding tissues and structures, and may eventually be lethal.
Examples
- Cervical squamous intraepithelial lesion (SIL), previously called cervical intraepithelial neoplasia (CIN), is a form of dysplasia that can progress to cervical cancer. The term carcinoma in situ may be used interchangeably with high-grade SIL.[8]
- Ductal carcinoma in situ of the breast is the most common precancer in women.
- Bowen's disease is a squamous carcinoma in situ of the skin.
- Colon polyps often contain areas of CIS that will almost always transform into colon cancer if left untreated.
- High-grade prostatic intraepithelial neoplasia is equivalent to CIS of the prostate.
- Bronchioloalveolar carcinoma (BAC) of the lung is the only form of CIS that can kill directly because, in rare cases (the "pneumonic form"), it expands greatly and fills the lungs, preventing breathing and causing other dire effects on the host. Thus, the pneumonic form of BAC is a true malignant entity, but is not "invasive" in the classical sense. For this reason, it is considered a form of CIS by pathologists, but not by oncologists or surgeons, and inclusion of this form of cancer among the types of CIS is controversial.
Treatment
Carcinoma in situ is, by definition, a localized phenomenon, with no potential for metastasis unless it progresses into cancer. Therefore, its removal eliminates the risk of subsequent progression into a life-threatening condition.
Some forms of CIS (e.g., colon polyps and polypoid tumours of the bladder) can be removed using an endoscope, without conventional surgical resection. Dysplasia of the uterine cervix is removed by excision (cutting it out) or by burning with a laser. Bowen's disease of the skin is removed by excision. Other forms require major surgery, the best known being intraductal carcinoma of the breast (also treated with radiotherapy). One of the most dangerous forms of CIS is the "pneumonic form" of BAC of the lung, which can require extensive surgical removal of large parts of the lung. When too large, it often cannot be completely removed, with eventual disease progression and death of the patient.
References
- 1 2 Chang, Alfred (2007). Oncology: An Evidence-Based Approach. Springer. p. 162. ISBN 9780387310565.
- ↑ "II Neoplams". World Health Organization. Retrieved 19 June 2014.
- ↑ Organization, World Health (2004). International statistical classification of diseases and related health problems (10. rev., 2. ed.). Geneva: World Health Organization. p. 38. ISBN 9789241546492.
- ↑ J.@Saclarides, ed. by Jonathan A.@Myers, Keith W.@Millikan, Theodore (2008). Common surgical diseases an algorithmic approach to problem solving. (2nd rev. ed.). New York: Springer. ISBN 9780387752464.
- ↑ Allred, DC (2010). "Ductal carcinoma in situ: terminology, classification, and natural history.". Journal of the National Cancer Institute. Monographs. 2010 (41): 134–8. doi:10.1093/jncimonographs/lgq035. PMID 20956817.
- ↑ Ridge JA, Glisson BS, Lango MN, et al. "Head and Neck Tumors" in Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ (Eds) Cancer Management: A Multidisciplinary Approach. 11 ed. 2008.
- ↑ "Cancer Staging Fact Sheet". National Cancer Institute. Retrieved June 24, 2014.
- ↑ "Understanding Cervical Changes" (PDF). National Cancer Institute. National Institute of Health. Retrieved 17 June 2014.