Alcohol and health

Short-term effects of alcohol consumption include intoxication and dehydration. Long-term effects of alcohol consumption include changes in the metabolism of the liver and brain and alcoholism. Alcohol intoxication affects the brain, causing slurred speech, clumsiness, and delayed reflexes. Alcohol stimulates insulin production, which speeds up glucose metabolism and can result in low blood sugar, causing irritability and possibly death for diabetics.[1] A 2014 World Health Organization report found that harmful alcohol consumption caused about 3.3 million deaths annually worldwide.[2]
However, some effects of alcohol consumption are beneficial. Although even moderate alcohol consumption increased the risk of death in younger people, it has been shown to decrease the risk of death for individuals ages 55+ (due to decreased risk of ischemic heart disease).[3]
The median lethal dose of alcohol in test animals is a blood alcohol content of 0.45%. This is about six times the level of ordinary intoxication (0.08%), but vomiting or unconsciousness may occur much sooner in people who have a low tolerance for alcohol.[4] The high tolerance of chronic heavy drinkers may allow some of them to remain conscious at levels above 0.40%, although serious health hazards are incurred at this level.
Alcohol also limits the production of vasopressin (ADH) from the hypothalamus and the secretion of this hormone from the posterior pituitary gland. This is what causes severe dehydration when alcohol is consumed in large amounts. It also causes a high concentration of water in the urine and vomit and the intense thirst that goes along with a hangover.
Stress, hangovers, and the oral contraceptive pill may increase the desire for alcohol because these things will lower the level of testosterone and alcohol will acutely elevate it.[5] Tobacco has the same effect of increasing the craving for alcohol.[6]
Short-term effects
The short-term effects of alcohol consumption range from a decrease in anxiety and motor skills at lower doses to unconsciousness, anterograde amnesia, and central nervous system depression at higher doses. Cell membranes are highly permeable to alcohol, so once alcohol is in the bloodstream it can diffuse into nearly every cell in the body.
The concentration of alcohol in blood is measured via blood alcohol content (BAC). The amount and circumstances of consumption play a large part in determining the extent of intoxication; for example, eating a heavy meal before alcohol consumption causes alcohol to absorb more slowly.[7] Hydration also plays a role, especially in determining the extent of hangovers. After excessive drinking, unconsciousness can occur and extreme levels of consumption can lead to alcohol poisoning and death (a concentration in the blood stream of 0.40% will kill half of those affected[8]). Alcohol may also cause death indirectly, by asphyxiation from vomit.
Alcohol can greatly exacerbate sleep problems. During abstinence, residual disruptions in sleep regularity and sleep patterns are the greatest predictors of relapse.[9]
Long-term effects
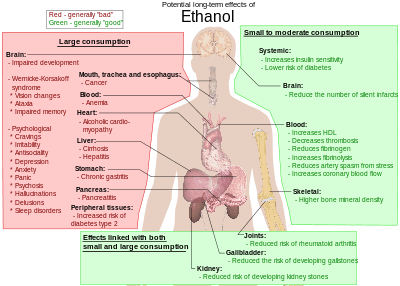
The long-term effects of alcohol consumption range from cardioprotective health benefits for low to moderate alcohol consumption in industrialized societies with higher rates of cardiovascular disease[10][11] to severe detrimental effects in cases of chronic alcohol abuse.[12] Health effects associated with large levels of alcohol intake include an increased risk of alcoholism, malnutrition, chronic pancreatitis, alcoholic liver disease and cancer. In addition, damage to the central nervous system and peripheral nervous system can occur from chronic alcohol abuse.[13][14] The long-term use of alcohol is capable of damaging nearly every organ and system in the body.[15] The developing adolescent brain is particularly vulnerable to the toxic effects of alcohol.[16] In addition, the developing fetal brain is also vulnerable, and fetal alcohol spectrum disorders (FASDs) may result if pregnant mothers consume alcohol.
Cardiovascular disease
A study published in the British Medical Journal on 10 July 2014 investigated the correlation between human variants of the ADH1B gene, which codes for the ADH1B enzyme (Alcohol dehydrogenase 1B), and cardiovascular health. The study concluded that carriers of one specific variant of this gene (A-allele of ADH1B rs1229984), which is associated with lower alcohol consumption, '...had a more favourable cardiovascular profile and a reduced risk of coronary heart disease than those without the genetic variant.' The study's authors extrapolated from this finding to suggest that '...reduction of alcohol consumption, even for light to moderate drinkers, is beneficial to health.'[17]
This study contradicts previous findings on the causal relationship between light alcohol consumption and cardiovascular health, and has been criticized on its methodology by members of the International Scientific Forum on Alcohol Research, which stated in its analysis that '...[there are] questions about making generalized statements about the effects of alcohol on disease based on results from the analysis of a single nucleotide polymorphism of a gene.'[18]
Moreover, the study fails to explain or discount previous findings that show a causal link between alcohol intake and cardiovascular health that can not be accounted for by genetic predisposition alone.[19]
Pregnancy
Medical organizations strongly discourage drinking alcohol during pregnancy.[20][21][22] Alcohol passes easily from the mother's bloodstream through the placenta and into the bloodstream of the fetus,[23] which interferes with brain and organ development.[24] Alcohol can affect the fetus at any stage during pregnancy, but the level of risk depends on the amount and frequency of alcohol consumed.[24] Regular heavy drinking and binge drinking (four or more drinks on any one occasion) pose the greatest risk for harm, but lesser amounts can cause problems as well.[24] There is no known safe amount or safe time to drink during pregnancy.[25]
Prenatal alcohol exposure can lead to fetal alcohol spectrum disorders (FASDs). The most severe form of FASD is fetal alcohol syndrome (FAS).[25] Problems associated with FASD include facial anomalies, low birth weight, stunted growth, small head size, delayed or uncoordinated motor skills, hearing or vision problems, learning disabilities, behavior problems, and inappropriate social skills compared to same-age peers.[26][27] Those affected are more likely to have trouble in school, legal problems, participate in high-risk behaviors, and develop substance use disorders themselves.[26]
Breastfeeding
The NHS states that minor amounts of alcohol do not make breastfeeding dangerous. However, it can be better to wait for a couple of hours before breastfeeding or express the milk into a bottle before drinking.[28] Researchers have shown that intoxicated breastfeeding reduces the average milk expression but poses no immediate threat to the child as the amount of transferred alcohol is insignificant.[29]
Alcohol expectations
Alcohol expectations are beliefs and attitudes that people have about the effects they will experience when drinking alcoholic beverages. They are just largely beliefs about alcohol's effects on a person’s behaviors, abilities, and emotions. Some people believe that if alcohol expectations can be changed, then alcohol abuse might be reduced. Men tend to become more aggressive in laboratory studies in which they are drinking only tonic water but believe that it contains alcohol. They also become less aggressive when they believe they are drinking only tonic water, but are actually drinking tonic water that contains alcohol.[30]
The phenomenon of alcohol expectations recognizes that intoxication has real physiological consequences that alter a drinker's perception of space and time, reduce psychomotor skills, and disrupt equilibrium.[31] The manner and degree to which alcohol expectations interact with the physiological short-term effects of alcohol, resulting in specific behaviors, is unclear.
A single study found that if a society believes that intoxication leads to sexual behavior, rowdy behavior, or aggression, then people tend to act that way when intoxicated. But if a society believes that intoxication leads to relaxation and tranquil behavior, then it usually leads to those outcomes. Alcohol expectations vary within a society, so these outcomes are not certain.[32]
People tend to conform to social expectations, and some societies expect that drinking alcohol will cause disinhibition. However, in societies in which the people do not expect that alcohol will disinhibit, intoxication seldom leads to disinhibition and bad behavior.[31]
Alcohol expectations can operate in the absence of actual consumption of alcohol. Research in the United States over a period of decades has shown that men tend to become more sexually aroused when they think they have been drinking alcohol, — even when they have not been drinking it. Women report feeling more sexually aroused when they falsely believe the beverages they have been drinking contained alcohol (although one measure of their physiological arousal shows that they became less aroused).
Drug treatment programs
Most addiction treatment programs encourage people with drinking problems to see themselves as having a chronic, relapsing disease that requires a lifetime of attendance at 12-step meetings to keep in check. However, some people do not develop lifelong problems.[33]
Alcohol abuse

Alcohol abuse prevention programs
The Army at Fort Drum has taken the "0-0-1-3" and exchanged it for the new "0-1-2-3" described in the Prime-For-Life Program, which highlights the ill effects of alcohol abuse as more than just an individual’s "driving while intoxicated." The Prime-For-Life program identifies alcohol abuse to be a health and impairment problem, leading to adverse legal as well as health outcomes associated with misuse.
The 0-1-2-3 now represents low-risk guidelines:
- 0 – Zero drinks for those driving a vehicle.
- 1 – One drink per hour
- 2 – No more than two drinking sessions per week
- 3 – Not to exceed three drinks on any one day
Recommended maximum intake
Binge drinking is becoming a major problem in the UK. Advice on weekly consumption is avoided in United Kingdom.[35]
Since 1995 the UK government has advised that regular consumption of three to four units a day for men and or two to three units for women, would not pose significant health risks. However, consistently drinking more than four units a day (for men) and three units (women), is not advisable.[36]
Previously (from 1992 until 1995), the advice was that men should drink no more than 21 units per week, and women no more than 14.[37] (The difference between the sexes was due to the typically lower weight and water-to-body-mass ratio of women.) This was changed because a government study showed that many people were in effect "saving up" their units and using them at the end of the week, a phenomenon referred to as binge drinking. The Times reported in October 2007 that these limits had been "plucked out of the air" and had no scientific basis.[38]
Sobriety
Sobriety is the condition of not having any measurable levels, or effects from mood-altering drugs. According to WHO "Lexicon of alcohol and drug terms..." sobriety is continued abstinence from psychoactive drug use.[39] Sobriety is also considered to be the natural state of a human being given at a birth. In a treatment setting, sobriety is the achieved goal of independence from consuming or craving mind-altering substances. As such, sustained abstinence is a prerequisite for sobriety. Early in abstinence, residual effects of mind-altering substances can preclude sobriety. These effects are labeled "PAWS", or "post acute withdrawal syndrome". Someone who abstains, but has a latent desire to resume use, is not considered truly sober. An abstainer may be subconsciously motivated to resume drug use, but for a variety of reasons, abstains (e.g. such as a medical or legal concern precluding use).[40] Sobriety has more specific meanings within specific contexts, such as the culture of Alcoholics Anonymous, other 12 step programs, law enforcement, and some schools of psychology. In some cases, sobriety implies achieving "life balance".[41]
Injury
Injury is defined as damage or harm that is done or sustained.[42] The potential of injuring yourself or others can be increased after consuming alcohol due to the certain short term effects related to the substance such as lack of coordination, blurred vision, and slower reflexes to name a few.[43] Due to these effects the most common injuries include head, fall, and vehicle related injuries. These include a range of soft tissue damage and fractures. A study was conducted between November 1, 2001 and June 30, 2002 of patients admitted to The Ulster Hospital in Northern Ireland with fall related injuries. They found that 113 of those patients admitted to that hospital during that had consumed alcohol recently and that the injury severity was higher for those that had consumed alcohol compared to those that hadn't.[44] Another study showed that 21% of patients admitted to the Emergency Department of the Bristol Royal Infirmary had either direct or indirect alcohol related injuries. If these figures are extrapolated it shows that the estimated number of patients with alcohol related injuries are over 7000 during the year at this ED alone.[45]
Genetic differences
Alcohol flush and respiratory reactions
Alcohol flush reaction is a condition in which an individual's face or body experiences flushes or blotches as a result of an accumulation of acetaldehyde, a metabolic byproduct of the catabolic metabolism of alcohol. It is best known as a condition that is experienced by people of Asian descent. According to the analysis by HapMap Project, the rs671 allele of the ALDH2 gene responsible for the flush reaction is rare among Europeans and Africans, and it is very rare among Mexican-Americans. 30% to 50% of people of Chinese and Japanese ancestry have at least one ALDH*2 allele.[46] The rs671 form of ALDH2, which accounts for most incidents of alcohol flush reaction worldwide, is native to East Asia and most common in southeastern China. It most likely originated among Han Chinese in central China,[47] and it appears to have been positively selected in the past. Another analysis correlates the rise and spread of rice cultivation in Southern China with the spread of the allele.[48] The reasons for this positive selection aren't known, but it's been hypothesized that elevated concentrations of acetaldehyde may have conferred protection against certain parasitic infections, such as Entamoeba histolytica.[49]
The same SNP allele of ALDH2, also termed glu487lys, and the abnormal accumulation of acetaldehyde following the drinking of alcohol, is associated with the alcohol-induced respiratory reactions of rhinitis and asthma that occur in Eastern Asian populations.[50]
![{\displaystyle {\ce {H}}{-}{\overset {\displaystyle {\ce {H}} \atop |}{\underset {| \atop \displaystyle {\ce {H}}}{\ce {C}}}}{-}{\overset {\displaystyle {\ce {H}} \atop |}{\underset {| \atop \displaystyle {\ce {H}}}{\ce {C}}}}{\ce {-O-H->[{\ce {ADH}}]H}}{-}{\overset {\displaystyle {\ce {H}} \atop |}{\underset {| \atop \displaystyle {\ce {H}}}{\ce {C}}}}{-}{\overset {\displaystyle {\ce {H}} \atop |}{\underset {\| \atop \displaystyle {\ce {O}}}{\ce {C}}}}{\ce {->[{\ce {ALDH}}]H}}{-}{\overset {\displaystyle {\ce {H}} \atop |}{\underset {| \atop \displaystyle {\ce {H}}}{\ce {C}}}}{-}{\overset {\color {white}{\displaystyle {\ce {H}} \atop |}}{\underset {\| \atop \displaystyle {\ce {O}}}{\ce {C}}}}{\ce {-O-H}}}](../I/m/8e29ab9d559420e2df0bf9ff99bef27374c71271.svg)
American Indian alcoholism
While little detailed genetic research has been done, it has been shown that alcoholism tends to run in families with possible involvement of differences in alcohol metabolism and the genotype of alcohol-metabolizing enzymes.
Genetics and amount of consumption
Having a particular genetic variant (A-allele of ADH1B rs1229984) is associated with non-drinking and lower alcohol consumption. This variant is also associated with favorable cardiovascular profile and a reduced risk of coronary heart disease compared to those without the genetic variant, but it is unknown whether this may be caused by differences in alcohol consumption or by additional confounding effects of the genetic variant itself.[51]
Gender differences
Alcoholism
Based on combined data from SAMHSA's 2004-2005 National Surveys on Drug Use & Health, the rate of past year alcohol dependence or abuse among people aged 12 or older varied by level of alcohol use: 44.7% of past month heavy drinkers, 18.5% binge drinkers, 3.8% past month non-binge drinkers, and 1.3% of those who did not drink alcohol in the past month met the criteria for alcohol dependence or abuse in the past year. Males had higher rates than females for all measures of drinking in the past month: any alcohol use (57.5% vs. 45%), binge drinking (30.8% vs. 15.1%), and heavy alcohol use (10.5% vs. 3.3%), and males were twice as likely as females to have met the criteria for alcohol dependence or abuse in the past year (10.5% vs. 5.1%).[52] Over time the difference between males and females has narrowed. According to a 2016 systematic review, for those born at the end of the 20th century men were 1.1 times as likely as women to drink alcohol at all, 1.2 times as likely to drink to problematic levels, and 1.3 times as likely to develop health problems from drinking.[53]
Sensitivity
Several biological factors make women more vulnerable to the effects of alcohol than men.[54]
- Body fat. Women tend to weigh less than men, and—pound for pound—a woman’s body contains less water and more fatty tissue than a man’s. Because fat retains alcohol while water dilutes it, alcohol remains at higher concentrations for longer periods of time in a woman’s body, exposing her brain and other organs to more alcohol.
- Enzymes. Women have lower levels of two enzymes—alcohol dehydrogenase and aldehyde dehydrogenase—that metabolize (break down) alcohol in the stomach and liver. As a result, women absorb more alcohol into their bloodstreams than men.
- Hormones. Changes in hormone levels during the menstrual cycle may also affect how a woman metabolizes alcohol.
Metabolism
Females demonstrated a higher average rate of elimination (mean, 0.017; range, 0.014-0.021 g/210 L) than males (mean, 0.015; range, 0.013-0.017 g/210 L). Female subjects on average had a higher percentage of body fat (mean, 26.0; range, 16.7-36.8%) than males (mean, 18.0; range, 10.2-25.3%).[55]
Depression
The link between alcohol consumption, depression, and gender was examined by the Centre for Addiction and Mental Health (Canada). The study found that women taking antidepressants consumed more alcohol than women who did not experience depression as well as men taking antidepressants. The researchers, Dr. Kathryn Graham and a PhD Student Agnes Massak analyzed the responses to a survey by 14,063 Canadian residents aged 18–76 years. The survey included measures of quantity, frequency of drinking, depression and antidepressants use, over the period of a year. The researchers used data from the GENACIS Canada survey, part of an international collaboration to investigate the influence of cultural variation on gender differences in alcohol use and related problems. The purpose of the study was to examine whether, like in other studies already conducted on male depression and alcohol consumption, depressed women also consumed less alcohol when taking anti-depressants.[56] According to the study, both men and women experiencing depression (but not on anti-depressants) drank more than non-depressed counterparts. Men taking antidepressants consumed significantly less alcohol than depressed men who did not use antidepressants. Non-depressed men consumed 436 drinks per year, compared to 579 drinks for depressed men not using antidepressants, and 414 drinks for depressed men who used antidepressants. Alcohol consumption remained higher whether the depressed women were taking anti-depressants or not. 179 drinks per year for non-depressed women, 235 drinks for depressed women not using antidepressants, and 264 drinks for depressed women who used antidepressants. The lead researcher argued that the study "suggests that the use of antidepressants is associated with lower alcohol consumption among men suffering from depression. But this does not appear to be true for women."[57]
See also
References
- ↑ http://www.mayoclinic.org/diseases-conditions/diabetes/expert-blog/alcohol-and-diabetes/BGP-20056464
- ↑ "Global status report on alcohol and health" (PDF). World Health Organization. 2014. pp. vii. Retrieved 23 November 2015.
- ↑ White IR; Altmann DR; Nanchahal K. (2000). "'Optimal' levels of alcohol consumption for men and women at different ages, and the all-cause mortality attributable to drinking." (PDF). London: London School of Hygiene and Tropical Medicine. Technical report.
- ↑ Meyer, Jerold S. and Linda F. Quenzer. Psychopharmacology: Drugs, the Brain, and Behavior. Sinauer Associates, Inc.: Sunderland, Massachusetts. 2005. Page 228.
- ↑ helsinki.fi - Effect of alcohol on hormones in women, Helsinki 2001
- ↑ helsinki.fi - Clinical studies on dependence and drug effects, ESBRA 2009
- ↑ Horowitz M, Maddox A, Bochner M, et al. (August 1989). "Relationships between gastric emptying of solid and caloric liquid meals and alcohol absorption". Am. J. Physiol. 257 (2 Pt 1): G291–8. PMID 2764113.
- ↑ Carleton College: Wellness Center: Blood Alcohol Concentration (BAC)
- ↑ Feige B, Scaal S, Hornyak M, Gann H, Riemann D (January 2007). "Sleep electroencephalographic spectral power after withdrawal from alcohol in alcohol-dependent patients". Alcohol. Clin. Exp. Res. 31 (1): 19–27. doi:10.1111/j.1530-0277.2006.00260.x. PMID 17207097.
- ↑ Association of alcohol consumption with selected cardiovascular disease outcomes: a systematic review and meta-analysis. Paul E Ronksley, Susan E Brien, Barbara J Turner, Kenneth J Mukamal, William A Ghali BMJ 2011;342:d671
- ↑ Prospective study of alcohol drinking patterns and coronary heart disease in women and men. Janne Tolstrup, Majken K Jensen, Tjønneland Anne, Kim Overvad, Kenneth J Mukamal, and Morten Grønbæk. BMJ 2006;332:1244.
- ↑ National Institute on Alcohol Abuse and Alcoholism (NIAAA) (2000). "Health risks and benefits of alcohol consumption" (PDF). Alcohol Res Health. 24 (1): 5–11. doi:10.4135/9781412963855.n839. PMID 11199274.
- ↑ Müller D, Koch RD, von Specht H, Völker W, Münch EM (March 1985). "Neurophysiologic findings in chronic alcohol abuse". Psychiatr Neurol Med Psychol (Leipz) (in German). 37 (3): 129–32. PMID 2988001.
- ↑ Testino G (2008). "Alcoholic diseases in hepato-gastroenterology: a point of view". Hepatogastroenterology. 55 (82–83): 371–7. PMID 18613369.
- ↑ Caan, Woody; Belleroche, Jackie de, eds. (11 April 2002). Drink, Drugs and Dependence: From Science to Clinical Practice (1st ed.). Routledge. pp. 19–20. ISBN 978-0-415-27891-1.
- ↑ Guerri,C.; Pascual,M.A. (2010)."Mechanisms involved in the neurotoxic, cognitive, and neurobehavioral effects of alcohol consumption during adolescence". Alcohol 44 (1) 15–26. doi:10.1016/j.alcohol.2009.10.003. PMID 20113871
- ↑ "Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data" (PDF). www.bmj.com. Retrieved 2015-02-04.
- ↑ "Critique 143: A Mendelian randomization assessment of alcohol and cardiovascular disease — 20 July 2014". Boston University. Retrieved 2015-01-12.
- ↑ King, Dana E., Mainous, III, Arch G. and Geesey, Mark E. (2008). "Adopting moderate alcohol consumption in middle-age: Subsequent cardiovascular events". American Journal of Medicine. 121 (3): 201–206. doi:10.1016/j.amjmed.2007.12.004.
- ↑ Vice Admiral Richard H. Carmona (2005). "A 2005 Message to Women from the U.S. Surgeon General" (PDF). Retrieved 12 June 2015.
- ↑ Committee to Study Fetal Alcohol Syndrome, Division of Biobehavioral Sciences and Mental Disorders, Institute of Medicine (1995). Fetal alcohol syndrome : diagnosis, epidemiology, prevention, and treatment. Washington, D.C.: National Academy Press. ISBN 0-309-05292-0.
- ↑ "Australian Government National Health and Medical Research Council". Retrieved 4 November 2012.
- ↑ Nathanson, Vivienne; Nicky Jayesinghe; George Roycroft (Oct 27, 2007). "Is it all right for women to drink small amounts of alcohol in pregnancy? No". BMJ. 335 (7625): 857. doi:10.1136/bmj.39356.489340.AD. PMC 2043444
 . PMID 17962287.
. PMID 17962287. - 1 2 3 "Fetal Alcohol Exposure". April 2015. Retrieved 10 June 2015.
- 1 2 "Facts about FASDs". April 16, 2015. Retrieved 10 June 2015.
- 1 2 Coriale; et al. (2013). "Fetal Alcohol Spectrum Disorder (FASD): neurobehavioral profile, indications for diagnosis and treatment.". Rivista di psichiatria. 48 (5): 359–69. doi:10.1708/1356.15062. PMID 24326748.
- ↑ Chudley; et al. (2005), "Fetal alcohol spectrum disorder: Canadian guidelines for diagnosis", CMAJ, 172 (5 Suppl): S1–S21, doi:10.1503/cmaj.1040302, PMC 557121, PMID 15738468, retrieved 16 April 2016
- ↑ http://www.nhs.uk/chq/pages/958.aspx?CategoryID=54&SubCategoryID=135#close
- ↑ Haastrup, Maija Bruun; Pottegård, Anton; Damkier, Per (February 2014). "Alcohol and Breastfeeding". Basic & Clinical Pharmacology & Toxicology. 114 (2): 168–173. doi:10.1111/bcpt.12149.
even in a theoretical case of binge drinking, the children would not be subjected to clinically relevant amounts of alcohol
- ↑ Grattan, Karen E.; Vogel-Sprott, M. (2001). "Maintaining Intentional Control of Behavior Under Alcohol". Alcoholism: Clinical and Experimental Research. 25 (2): 192–7. doi:10.1111/j.1530-0277.2001.tb02198.x. PMID 11236832.
- 1 2 MacAndrew, C. and Edgerton. Drunken Comportment: A Social Explanation. Chicago: Aldine, 1969.
- ↑ Marlatt GA, Rosenow (1981). "The think-drink effect". Psychology Today. 15: 60–93.
- ↑ Szalavitz, Maia (14 May 2012). "DSM-5 Could Categorize 40% of College Students as Alcoholics". Time. Retrieved 31 January 2015.
- ↑ Nutt, D; King, LA; Saulsbury, W; Blakemore, C (24 March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse.". Lancet (London, England). 369 (9566): 1047–53. doi:10.1016/S0140-6736(07)60464-4. PMID 17382831.
- ↑ "Sensible Drinking". Aim-digest.com. Retrieved 2013-02-05.
- ↑ "Alcohol misuse : Department of Health". Dh.gov.uk. Retrieved 2013-02-05.
- ↑ "Alcohol and health: how alcohol can affect your long and short term health". Drinkaware.co.uk. Archived from the original on 21 April 2009. Retrieved 2013-02-05.
- ↑ Drink limits ‘useless’, The Times, 20 October 2007
- ↑ "Lexicon and drug terms". Who.int. 2010-12-09. Retrieved 2013-02-05.
- ↑ MD Basharin K.G. (2010). "Scientific grounding for sobriety: Western experience" (PDF). Retrieved 2013-02-05.
- ↑ "TWELVE STEPS and TWELVE TRADITIONS"
- ↑ "Dictionary.com".
- ↑ "Drinkwise Australia". DrinkWise Australia.
- ↑ McGovern & Johnston (26 July 2003). "Alcohol related falls: an interesting pattern of injuries".
- ↑ Rebecca Hoskins; Jonathan Benger (2013). "What is the burden of alcohol-related injuries in an inner city emergency department?". Alcoholism: Clinical and Experimental Research. 33: 1532–1538. doi:10.1111/j.1530-0277.2009.00981.x.
- ↑ "Rs671".
- ↑ Hui Li; et al. (2009). "Refined Geographic Distribution of the Oriental ALDH2*504Lys (nee 487Lys) Variant". Ann Hum Genet. 73 (Pt 3): 335–45. doi:10.1111/j.1469-1809.2009.00517.x. PMC 2846302. PMID 19456322.
- ↑ Yi Peng; Hong Shi; Xue-bin Qi; Chun-jie Xiao; Hua Zhong; Run-lin Z Ma; Bing Su (2010). "The ADH1B Arg47His polymorphism in East Asian populations and expansion of rice domestication in history". BMC Evolutionary Biology. 10 (1): 15. doi:10.1186/1471-2148-10-15. PMC 2823730. PMID 20089146.
- ↑ Oota; et al. (2004). "The evolution and population genetics of the ALDH2 locus: random genetic drift, selection, and low levels of recombination". Annals of Human Genetics. 68: 93–109. doi:10.1046/j.1529-8817.2003.00060.x.
- ↑ Adams, Karla E.; Rans, Tonya S. (December 2013). "Adverse reactions to alcohol and alcoholic beverages". Annals of Allergy, Asthma & Immunology. 111 (6): 439–445. doi:10.1016/j.anai.2013.09.016. PMID 24267355.
- ↑ Michael; et al. (2014). "Association between alcohol and cardiovascular disease: Mendelian randomisation analysis based on individual participant data". BMJ. 349: g4164. doi:10.1136/bmj.g4164.
- ↑ "Gender differences in alcohol use and alcohol dependence or abuse: 2004 or 2005." The NSDUH Report.Accessed June 22, 2012.
- ↑ Slade, Tim; Chapman, Cath; Swift, Wendy; Keyes, Katherine; Tonks, Zoe; Teesson, Maree (24 October 2016). "Birth cohort trends in the global epidemiology of alcohol use and alcohol-related harms in men and women: systematic review and metaregression". BMJ Open. 6 (10): e011827. doi:10.1136/bmjopen-2016-011827.
- ↑ "Women & Alcohol: The Hidden Risks of Drinking". Helpguide.org. Retrieved 2013-02-05.
- ↑ "Determination of volume of distribution for ethanol in male and female subjects.". J Anal Toxicol. 20 (5): 287–90. Sep 1996. doi:10.1093/jat/20.5.287. PMID 8872236.
- ↑ "Antidepressants Help Men, But Not Women, Decrease Alcohol Consumption." Science Daily. Feb. 27, 2007.
- ↑ Graham, Katherine and Massak, Agnes. "Alcohol consumption and the use of antidepressants." UK Pubmed Central (2007). June 20, 2012.