Angiostrongylus cantonensis
| Angiostrongylus cantonensis | |
|---|---|
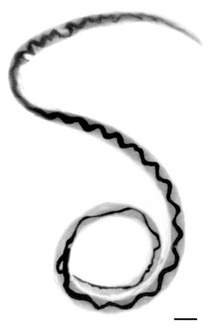 | |
| Adult female worm of Angiostrongylus cantonensis with characteristic barber-pole appearance (anterior end of worm is to the top). Scale bar is 1 mm. | |
| Scientific classification | |
| Kingdom: | Animalia |
| Phylum: | Nematoda |
| Class: | Secernentea |
| Order: | Strongylida |
| Family: | Metastrongylidae |
| Genus: | Angiostrongylus |
| Species: | A. cantonensis |
| Binomial name | |
| Angiostrongylus cantonensis (Chen, 1935) [1] | |
Angiostrongylus cantonensis is a parasitic nematode (roundworm) that causes angiostrongyliasis, the most common cause of eosinophilic meningitis in Southeast Asia and the Pacific Basin.[2] The nematode commonly resides in the pulmonary arteries of rats, giving it the nickname the rat lungworm. Snails are the primary intermediate hosts, where larvae develop until they are infective.
Humans are incidental hosts of this roundworm, and may become infected through ingestion of larvae in raw or undercooked snails or other vectors, or from contaminated water and vegetables. The larvae are then transported via the blood to the central nervous system (CNS), where they are the most common cause of eosinophilic meningitis, a serious condition that can lead to death or permanent brain and nerve damage.[3] Angiostrongyliasis is an infection of increasing public health importance as globalization contributes to the geographic spread of the disease.
History
First described by Chen (1935)[1] in Cantonese rats, the nematode Angiostrongylus cantonensis was identified in the cerebrospinal fluid of a patient with eosinophilic meningitis by Nomura and Lim in Taiwan in 1944. They noted that raw food eaten by the patient may have been contaminated by rats. In 1955, Mackerass and Sanders identified the life cycle of the worm in rats, defining snails and slugs as the intermediate host and noting the path of transmission through the blood, brain, and lungs in rats.
In 2013, A. cantonensis was confirmed present in Florida, USA, where its range and prevalence are expanding.[4]
Infectious agent

Angiostrongylus cantonensis is a helminth of the phylum Nematoda, order Strongylida, and superfamily Metastrongyloidea. Nematodes are roundworms characterized by a tough outer cuticle, unsegmented bodies, and a fully developed gastrointestinal tract. The order Strongylida includes hookworms and lungworms. Metastrongyloidea are characterized as long, slender, threadlike worms that reside in the lungs of the definitive host.[5] Angiostrongylus costaricensis is a closely related worm that causes intestinal Angiostrongyliasis in Central and South America.
Epidemiology
Following World War II, A. cantonensis spread throughout Southeast Asia and Western Pacific Islands including Australia, Melanesia, Micronesia, and Polynesia. Cases were soon reported in the following nations: New Caledonia, the Philippines, Rarotonga, Saipan, Sumatra, Taiwan and Tahiti. In the 1960s even more cases were reported from the region from locations such as: Cambodia, Guam, Hawaii, Java, Thailand, Sarawak, Vietnam and the New Hebrides (Vanuatu).[6]
In 1961, an epidemiological study of eosinophilic meningitis in humans was conducted by Rosen, Laigret, and Bories, who hypothesized that the parasite causing these infections was carried by fish. However Alicata noted that raw fish was consumed by large numbers of people in Hawaii without apparent consequences, and patients presenting with meningitis symptoms had a history of eating raw snails or prawns in the weeks before presenting with symptoms. This observation along with epidemiology and autopsy of infected brains confirmed A. cantonensis infection in humans as the cause of the majority of eosinophilic meningitis cases in Southeast Asia and the Pacific Islands.[7]
Since then, cases of A. cantonensis infestations have appeared in American Samoa, Australia, Hong Kong, Bombay, Fiji, Hawaii, Honshu, India, Kyushu, New Britain, Okinawa, Ryukyu Islands, Western Samoa and most recently mainland China. Other sporadic occurrences of the parasite in its rat hosts have been reported in Cuba, Egypt, Louisiana, Madagascar, Nigeria, New Orleans and Puerto Rico[6]
In recent years, the parasite has been shown to be proliferating at an alarming rate due to modern food consumption trends and global transportation of food products. Scientists are calling for a more thorough study of the epidemiology of A. cantonensis, stricter food safety policies, and the increase of knowledge on how to properly consume products commonly infested by the parasite.[8]
Hosts
Intermediate hosts of larvae of for Angiostrongylus cantonensis include:
- land snails: Thelidomus aspera from Jamaica,[9] Achatina fulica,[8][10][11][12] Satsuma mercatoria,[11][12] Acusta despecta,[11][12] Bradybaena brevispira,[8] Bradybaena circulus[11] Bradybaena ravida,[8] Bradybaena similaris,[8] Plectotropis appanata[8] and Parmarion martensi from Okinawa[11] and from Hawaii,[13] Camaena cicatricosa,[8] Trichochloritis rufopila,[8] Trichochloritis hungerfordianus[8] and Cyclophorus spp.[12]
- freshwater snails: Pila spp.,[10] Pomacea canaliculata,[8][10] Cipangopaludina chinensis,[8] Bellamya aeruginosa[8] and Bellamya quadrata[8]
- slugs: Limax maximus,[14] Limax flavus[8] Deroceras laeve,[8][15] Deroceras reticulatum,[15] Veronicella alte,[11] =? Laevicaulis alte,[8][15] Sarasinula plebeia,[15] Vaginulus yuxjsjs,[8] Lehmannia valentiana,[11] Phiolomycus bilineatus,[8] Macrochlamys loana,[8] Meghimatium bilineatum[8] and probably other species of slugs.
Definitive host of Angiostrongylus cantonensis include wild rodents, especially the brown rat (Rattus norvegicus)[9] and the black rat (Rattus rattus).[9]
Paratenic hosts of Angiostrongylus cantonensis include: predatory land flatworm Platydemus manokwari[11] and amphibians Bufo asiaticus,[11] Rana catesbeiana,[11] Rhacophorus leucomystax[11] and Rana limnocharis.[11]
In 2004, a captive yellow-tailed black cockatoo (Calyptorhynchus funereus) and two free-living tawny frogmouths (Podargus strigoides) suffering neurological symptoms were shown to have the parasite. They were the first non-mammalian hosts discovered for the organism.[16]
Pathogenesis of human angiostrongylosis
The presence of parasitic worms burrowed in the neural tissue of the human CNS will cause obvious complications. All of the following will result in damage to the CNS:
- Direct mechanical damage to neural tissue from the worms' motion
- Toxic by-products such as nitrogenous waste
- Antigens released by dead and living parasites
Eosinophilic meningitis
Although the clinical disease caused by Angiostrongylus invasion into the central nervous system is commonly referred to as "eosinophilic meningitis", the actual pathophysiology is of a meningoencephalitis with invasion not just of the meninges, or superficial lining of the brain, but also deeper brain tissue. Initial invasion through the lining of the brain, the meninges, may cause a typical inflammation of the meninges and a classic meningitis picture of headache, stiff neck and often fever. The parasites subsequently invade deeper into the brain tissue, causing specific localizing neurologic symptoms depending on where in the brain parenchyma they migrate. Neurologic findings and symptoms wax and wane as initial damage is done by the physical in-migration of the worms and secondary damage is done by the inflammatory response to the presence of dead and dying worms. This inflammation can lead in the short term to paralysis, bladder dysfunction, visual disturbance and coma and in the long term to permanent nerve damage, mental retardation, nerve damage, permanent brain damage or death.
Eosinophilic meningitis is commonly defined by the increased number of eosinophils in the cerebrospinal fluid (CSF). In most cases, eosinophil levels rise to 10 or more eosinophils per μL in the cerebrospinal fluid, accounting for at least 10% of the total CSF leukocyte count.[6] The chemical analysis of the CSF typically resembles the findings in "aseptic meningitis" with slightly elevated protein levels, normal glucose levels and negative bacterial cultures. Presence of a significantly decreased glucose on CSF analysis is an indicator of severe meningoencephalitis and may indicate a poor prognosis. Initial CSF analysis early in the disease process may occasionally show no increase of eosinophils only to have classical increases in eosinophils in subsequent spinal fluid analysis. Caution should be advised in using eosinophilic meningitis as the only criterion for diagnosing angiostrongylus infestation in someone with classic symptoms as the disease evolves with the migration of the worms into the central nervous system.
Eosinophils are specialized white blood cells of the granulocytic cell line which contain granules in their cytoplasm. These granules contain proteins that are toxic to parasites. When these granules degranulate, or break down, chemicals are released that combat parasites such as A. cantonensis. Eosinophils, which are located throughout the body, are guided to sites of inflammation by chemokines when the body is infested with parasites such as A. cantonensis. Once at the site of inflammation, Type 2 cytokines are released from helper T cells, which communicate with the eosinophils, signaling them to activate. Once activated, eosinophils can begin the process of degranulation, releasing their toxic proteins in the fight against the foreign parasite.
Clinical symptoms
The clinical symptoms of eosinophilic meningitis are as follows:
- fever is often minor or absent but the presence of high fever suggests severe disease.
- headaches- a bitemporal character in the frontal or occipital lobe
- meningismus - neck stiffness
- photophobia - sensitivity to light
- nausea with or without vomiting
- paresthesias - tingling, prickling, or numbing of skin
- hyperesthesia - severe sensitivity to touch
- bladder dysfunction with urinary retention
- vertigo
- blindness[6]
- paralysis localized to one area
- general paralysis often ascending in nature starting with the feet and progressing upwards to involve the entire body.
- coma
- death
Treatment
The severity and clinical course of Angiostrongylus disease depends significantly on the ingested load of third-stage larvae,[17] creating great variability from case to case making it difficult to design clinical trials and to judge the effectiveness of treatments. Typical conservative medical management including analgesics and sedatives provide minimal relief the headaches and hyperesthesias. Removing cerebrospinal fluid at regular three- to seven-day intervals is the only proven method of significantly reducing intracranial pressure and can be used for symptomatic treatment of headaches. This process may be repeated until improvement is shown.[6] Recent studies have shown that treatment with an antihelminthic such as mebendazole or albendazole combined with prednisone or prednisolone can reduce the severity and duration of headaches but have not been shown to improve long-term neurologic outcomes.
Diagnosis
The diagnosis of disease caused by Angiostrongylus cantonensis infestation is often difficult and relies heavily on the history of a likely ingestion of a commonly infested host and the presence of typical features of the disease. The presumptive diagnosis is particularly strong when eospinophilic meningoencephalitis can be confirmed. The diagnosis of eosinophilic meningitis can be arrived at through detection of elevated cranial pressure and increased numbers of eosinophils. The diagnosis of the cause of eosinophilic meningitis and the presence of A. cantonensis is remarkably more difficult. A spinal tap, or a sample of CSF, must be taken to search for A. cantonensis worms or larvae. A. cantonensis is undetectable in the CSF of more than half of the infected individuals. Current methods of detecting specific antigens associated with A. cantonensis are also unreliable. Consequently, alternative approaches to detect antigen-antibody reactions are being explored, such as Immuno-PCR.[18]
References
- 1 2 Chen, HT (1935). "Un nouveau nématode pulmonaire, Pulmonema cantonensis n.g., n.sp., des rats de Canton". Annales de Parasitologie Humaine et Comparée. 13: 312–317.
- ↑ Baheti, N. N.; Sreedharan, M.; Krishnamoorthy, T.; Nair, M. D.; Radhakrishnan, K. (2008). "Eosinophilic meningitis and an ocular worm in a patient from Kerala, south India". Journal of Neurology, Neurosurgery & Psychiatry. 79 (3): 271. doi:10.1136/jnnp.2007.122093. PMID 18281446.
- ↑ Li, H.; Xu, F.; Gu, J. B.; Chen, X. G. (2008). "A severe eosinophilic meningoencephalitis caused by infection of Angiostrongylus cantonensis". The American journal of tropical medicine and hygiene. 79 (4): 568–570. PMID 18840746.
- ↑ Iwanowicz DD, Sanders LR, Schill WB, Xayavong MV, da Silva AJ, Qvarnstrom Y, Smith T. 2015. Spread of the Rat Lungworm (Angiostrongylus cantonensis) in Giant African Land Snails (Lissachatina fulica) in Florida, USA. Journal of Wildlife Diseases 51(3):749-53. doi: 10.7589/2014-06-160. Epub 2015 May 14.
- ↑ "Helminth Taxonomy - Phylum Nematoda" Archived April 13, 2009, at the Wayback Machine., Schistosomiasis Research Group, accessed 26 February 2009.
- 1 2 3 4 5 "EOSINOPHILIC MENINGITIS". Revised 28 February 2006, accessed 1 June 2011.
- ↑ Alicata, J. E. (1991). "The Discovery of Angiostrongylus cantonensis as a Cause of Human Eosinophilic Meningitis". Parasitology Today. 7 (6): 151–153. doi:10.1016/0169-4758(91)90285-v.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Lv S., Zhang Y., Steinmann P. &, Zhou X.-N. (2008). "Emerging angiostrongyliasis in mainland China". Emerging Infectious Diseases 14(1): 161-164. HTM.
- 1 2 3 Lindo J. F., Waugh C., Hall J., Cunningham-Myrie C., Ashley D., Eberhard M. L., Sullivan J. J., Bishop H. S., Robinson D. G., Holtz T. & Robinson R. D. (2002). "Enzootic Angiostrongylus cantonensis in Rats and Snails after an Outbreak of Human Eosinophilic Meningitis, Jamaica". Emerging Infectious Diseases 8(3): 324-326. HTM.
- 1 2 3 Lv, S.; Zhang, Y.; Chen, S. R.; Wang, L. B.; Fang, W.; Chen, F.; Jiang, J. Y.; Li, Y. L.; Du, Z. W.; Zhou, X. N. (2009). Graeff-Teixeira, Carlos, ed. "Human Angiostrongyliasis Outbreak in Dali, China". PLoS Neglected Tropical Diseases. 3 (9): e520. doi:10.1371/journal.pntd.0000520. PMC 2739427
 . PMID 19771154.
. PMID 19771154. - 1 2 3 4 5 6 7 8 9 10 11 12 Asato R., Taira K., Nakamura M., Kudaka J., Itokazu K. & Kawanaka M. (2004) "Changing Epidemiology of Angiostrongyliasis Cantonensis in Okinawa Prefecture, Japan". Japanese Journal of Infectious Diseases 57: 184-186. article Archived October 13, 2008, at the Wayback Machine.
- 1 2 3 4 (20 June 2001). "Land snail infection rates for the human parasitic nematode, Angiostrongylus cantonensis (rat lung worm) with notes on snail and parasite biology and distribution on Kadena AB, Okinawa Japan. Consultative Letter, IERA-DO-BR-CL-2001-0049." MEMORANDUM FOR 18 MDG/SGPM, Department of the Air Force, 11 pp. PDF Archived August 11, 2011, at the Wayback Machine..
- ↑ Hollingsworth, R. G.; Kaneta, R.; Sullivan, J. J.; Bishop, H. S.; Qvarnstrom, Y.; Da Silva, A. J.; Robinson, D. G. (2007). "Distribution of Parmarion cf. Martensi (Pulmonata: Helicarionidae), a New Semi-Slug Pest on Hawai'i Island, and Its Potential as a Vector for Human Angiostrongyliasis1". Pacific Science. 61 (4): 457–467. doi:10.2984/1534-6188(2007)61[457:DOPCMP]2.0.CO;2..
- ↑ Senanayake, S. N.; Pryor, D. S.; Walker, J.; Konecny, P. (2003). "First report of human angiostrongyliasis acquired in Sydney". The Medical journal of Australia. 179 (8): 430–431. PMID 14558868.
- 1 2 3 4 Högger C. H. (update 25 March 2003). "Antagonists of Slugs and Snails. A Bibliography of Sources and a List of Citations grouped according to Taxon of the Antagonists". in web Archive.
- ↑ Monks, D. J.; Carlisle, M. S.; Carrigan, M.; Rose, K.; Spratt, D.; Gallagher, A.; Prociv, P. (2005). "Angiostrongylus cantonensis as a Cause of Cerebrospinal Disease in a Yellow-tailed Black Cockatoo (Calyptorhynchus funereus) and Two Tawny Frogmouths (Podargus strigoides)". Journal of Avian Medicine and Surgery. 19 (4): 289–293. doi:10.1647/2004-024.1.
- ↑ Tsai, H. C.; Liu, Y. C.; Kunin, C. M.; Lee, S. S.; Chen, Y. S.; Lin, H. H.; Tsai, T. H.; Lin, W. R.; Huang, C. K.; Yen, M. Y.; Yen, C. M. (2001). "Eosinophilic meningitis caused by Angiostrongylus cantonensis: Report of 17 cases". The American Journal of Medicine. 111 (2): 109–114. doi:10.1016/S0002-9343(01)00766-5. PMID 11498063.
- ↑ Chye, S. -M.; Lin, S. R.; Chen, Y. L.; Chung, L. Y.; Yen, C. M. (2004). "Immuno-PCR for Detection of Antigen to Angiostrongylus cantonensis Circulating Fifth-Stage Worms". Clinical Chemistry. 50 (1): 51–57. doi:10.1373/clinchem.2003.020867. PMID 14709636.
External links
| Wikimedia Commons has media related to Angiostrongylus cantonensis. |
- Division of Parasitic Diseases, Centers for Disease Control and Prevention, Angiostrongylus cantonensis Infection
- Laboratory Identification of Parasites of Public Health Concern, Parasites and Health, Angiostrongyliasis
- Laboratory Identification of Parasites of Public Health Concern, Angiostrongyliasis Image Library
- Angiostrongylus cantonensis at the US National Library of Medicine Medical Subject Headings (MeSH)
- Sydney Morning Herald story of human infection, Example of Angiostrongylus cantonensis human infection: Hard to swallow: slug-eating dare causes rare disease
- Angiostronglyus cantonensis on the UF / IFAS Featured Creatures website.