Chlamydophila psittaci
| Chlamydia psittaci | |
|---|---|
 | |
| Direct fluorescent antibody stain of a mouse brain impression smear showing C. psittaci. | |
| Scientific classification | |
| Kingdom: | Bacteria |
| Phylum: | Chlamydiae |
| Order: | Chlamydiales |
| Family: | Chlamydiaceae |
| Genus: | Chlamydia |
| Species: | C. psittaci |
| Binomial name | |
| Chlamydia psittaci[1] | |
Chlamydia psittaci is a lethal intracellular bacterial species that may cause endemic avian chlamydiosis, epizootic outbreaks in mammals, and respiratory psittacosis in humans. Potential hosts include feral birds and domesticated poultry as well as cattle, pigs, sheep and horses. Chlamydia psittaci is transmitted by inhalation, contact or ingestion among birds and to mammals. Psittacosis in birds and in humans often starts with flu-like symptoms and becomes a life-threatening pneumonia. Many strains remain quiescent in birds until activated under stress. Birds are excellent, highly mobile vectors for the distribution of chlamydia infection, because they feed on, and have access to, the detritus of infected animals of all sorts.
Chlamydia psittaci was previously classified as Chlamydophila psittaci. The former "mammalian" Chlamydia psittaci abortion, feline and Guinea pig strains have been moved to three new species. (See Chlamydia abortus, Chlamydia felis and Chlamydia caviae.)
C. psittaci in birds is often systemic and infections can be inapparent, severe, acute or chronic with intermittent shedding.[2][3][4][5] C. psittaci strains in birds infect mucosal epithelial cells and macrophages of the respiratory tract. Septicaemia eventually develops and the bacteria become localized in epithelial cells and macrophages of most organs, conjunctiva, and gastrointestinal tract. It can also be passed in the eggs. Stress will commonly trigger onset of severe symptoms, resulting in rapid deterioration and death. C. psittaci strains are similar in virulence, grow readily in cell culture, have 16S rRNA genes that differ by <0.8%, and belong to eight known serotypes. All should be considered to be readily transmissible to humans.
C. psittaci serovar A is endemic among psittacine birds and has caused sporadic zoonotic disease in humans, other mammals and tortoises. Serovar B is endemic among pigeons, has been isolated from turkeys, and has also been identified as the cause of abortion in herds of dairy cattle. Serovars C and D are occupational hazards for slaughterhouse workers and for people in contact with birds. Serovar E isolates (known as Cal-10, MP or MN) have been obtained from a variety of avian hosts worldwide and, although they were associated with the 1920s–1930s outbreak in humans, a specific reservoir for serovar E has not been identified. The M56 and WC serovars were isolated during outbreaks in mammals. Many C. psittaci strains are susceptible to bacteriophages.
Life cycle and method of infection
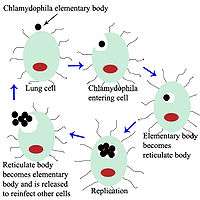
Chlamydia psittaci is a small bacterium (0.5 micrometres) that undergoes several transformations during its life cycle. It exists as an elementary body (EB) in between hosts. The EB is not biologically active, but is resistant to environmental stresses and can survive outside a host. The EB travels from an infected bird to the lungs of an uninfected bird or person in small droplets, and is responsible for infection. Once in the lungs, the EB is taken up by cells in a pouch called an endosome by a process called phagocytosis. However, the EB is not destroyed by fusion with lysosomes, as is typical for phagocytosed material. Instead, it transforms into a reticulate body and begins to replicate within the endosome. The reticulate bodies must use some of the host's cellular machinery to complete its replication. The reticulate bodies then convert back to elementary bodies, and are released back into the lung, often after causing the death of the host cell. The EBs are thereafter able to infect new cells, either in the same organism or in a new host. Thus, the life cycle of C. psittaci is divided between the elementary body which is able to infect new hosts, but can not replicate, and the reticulate body, which replicates, but is not able to cause new infection.
History
The disease caused by C. psittaci, psittacosis, was first characterized in 1879 when seven individuals in Switzerland were found to experience pneumonia after exposure to tropical pet birds. The related bacterial species Chlamydia trachomatis was described in 1907, but was assumed to be a virus, as it could not be grown on artificial media. In the winter of 1929–1930, a psittacosis pandemic spread across the United States and Europe. Its mortality rate was 20% and as high as 80% for pregnant women. The disease's spread was eventually attributed to exposure to Amazon parrots imported from Argentina. Though C. psittaci was identified in 1930 as the agent responsible for psittacosis, it was not found to be a bacterium until examination by electron microscopy in the 1960s.[6]
Confirmation of diagnosis
In addition to symptoms and CHX, complement fixation, microimmunofluorescence and PCR tests can be used to confirm the diagnosis.
Treatment
Tetracycline or macrolides can be used to treat this condition. The drugs are given intravenously or orally, depending on drug choice. Treatment should continue for 10–14 days after the fever subsides. In children or pregnant women, though, tetracycline should not be used. Ibuprofen or acetominophen, and fluids are also administered. Cigarette or tobacco smoke should be avoided. While taking tetracycline, dairy products should be avoided.
See also
References
- ↑ Everett, K. D. E.; Bush, R. M.; Andersen, A. A. (1999). "Emended description of the order Chlamydiales, proposal of Parachlamydiaceae fam. nov. and Simkaniaceae fam. nov., each containing one monotypic genus, revised taxonomy of the family Chlamydiaceae, including a new genus and five new species, and standards for the identification of organisms". International Journal of Systematic Bacteriology. 49 (2): 415–440. doi:10.1099/00207713-49-2-415. ISSN 0020-7713. PMID 10319462.
- ↑ http://www.chlamydiae.com/docs/Chlamydiales/genus_chlamydophila.asp
- ↑ Andersen AA (September 2005). "Serotyping of US isolates of Chlamydophila psittaci from domestic and wild birds". J. Vet. Diagn. Invest. 17 (5): 479–82. doi:10.1177/104063870501700514. PMID 16312243.
- ↑ Dorrestein GM, Wiegman LJ (December 1989). "[Inventory of the shedding of Chlamydia psittaci by parakeets in the Utrecht area using ELISA]". Tijdschr Diergeneeskd (in Dutch and Flemish). 114 (24): 1227–36. PMID 2617495.
- ↑ Sareyyupoglu B, Cantekin Z, Bas B (2007). "Chlamydophila psittaci DNA detection in the faeces of cage birds". Zoonoses Public Health. 54 (6–7): 237–42. doi:10.1111/j.1863-2378.2007.01060.x. PMID 17803512.
- ↑ Harkinezhad, Taher; Geens, Tom; Vanrompay, Daisy (1 March 2009). "Chlamydophila psittaci infections in birds: A review with emphasis on zoonotic consequences". Veterinary Microbiology. 135 (1-2): 68–77. doi:10.1016/j.vetmic.2008.09.046.
Further reading
- Brock Biology of Microorganisms (10th ed.). Upper Saddle River, NJ: Prentice Hall. 2003. ISBN 0-13-049147-0.