Foreign body in alimentary tract
| Foreign body in alimentary tract | |
|---|---|
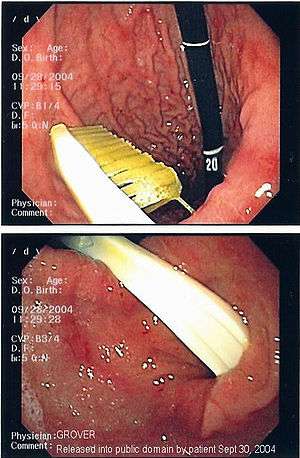 | |
| Endoscopy image of gastric foreign body (toothbrush) | |
| Classification and external resources | |
| Specialty | emergency medicine |
| ICD-10 | T18 |
| ICD-9-CM | 935-938 |
One of the most common locations for a foreign body is the alimentary tract.
It is possible for foreign bodies to enter the tract from the mouth,[1] or from the rectum.[2]
The objects most commonly swallowed by children are coins.[3] Meat impaction is more common in adults.[4]
Swallowed objects are more likely to lodge in the esophagus or stomach than in the pharynx or duodenum.[5]
Diagnosis
If the person who swallowed the foreign body is doing well, usually an x-ray image will be taken which will show any metal objects, and this will be repeated a few days later to confirm that the object has passed all the way through the digestive system. Also it needs to be confirmed that the object is not stuck in the airways, in the bronchial tree.
Treatment
Most objects that are swallowed will, if they have passed the pharynx, pass all the way through the gastrointestinal tract unaided.[6]
However, sometimes an object becomes arrested (usually in the terminal ileum or the rectum) or a sharp object penetrates the bowel wall.
If the foreign body causes problems like pain, vomiting or bleeding it must be removed.
Swallowed batteries can be associated with additional damage,[7][8] with mercury poisoning (from mercury batteries) and lead poisoning (from lead batteries) presenting important risks.
One technique used is endoscopic foreign body retrieval.
Additional images
 Abdominal X-ray showing small packages of cocaine swallowed by a trafficker.
Abdominal X-ray showing small packages of cocaine swallowed by a trafficker.
 Chest radiograph showing a Venezuelan 25 cent coin lodged in the upper esophagus of a 9-year-old girl.
Chest radiograph showing a Venezuelan 25 cent coin lodged in the upper esophagus of a 9-year-old girl. A coin seen on AP CXR in the esophagus
A coin seen on AP CXR in the esophagus A coin seen on lateral CXR in the esophagus
A coin seen on lateral CXR in the esophagus Fishbone pierced in the upper esophagus.Left image during swallowing contrast medium, right image after swallow only dimly visible.
Fishbone pierced in the upper esophagus.Left image during swallowing contrast medium, right image after swallow only dimly visible.
See also
References
- ↑ "Pediatrics, Foreign Body Ingestion: Overview - eMedicine". Retrieved 2008-12-18.
- ↑ Koornstra JJ, Weersma RK (July 2008). "Management of rectal foreign bodies: description of a new technique and clinical practice guidelines". World J. Gastroenterol. 14 (27): 4403–6. doi:10.3748/wjg.14.4403. PMC 2731197
 . PMID 18666334.
. PMID 18666334. - ↑ Arana A, Hauser B, Hachimi-Idrissi S, Vandenplas Y (August 2001). "Management of ingested foreign bodies in childhood and review of the literature". Eur. J. Pediatr. 160 (8): 468–72. doi:10.1007/s004310100788. PMID 11548183.
- ↑ Conway WC, Sugawa C, Ono H, Lucas CE (March 2007). "Upper GI foreign body: an adult urban emergency hospital experience". Surg Endosc. 21 (3): 455–60. doi:10.1007/s00464-006-9004-z. PMID 17131048.
- ↑ Li ZS, Sun ZX, Zou DW, Xu GM, Wu RP, Liao Z (October 2006). "Endoscopic management of foreign bodies in the upper-GI tract: experience with 1088 cases in China". Gastrointest. Endosc. 64 (4): 485–92. doi:10.1016/j.gie.2006.01.059. PMID 16996336.
- ↑ Lin CH, Chen AC, Tsai JD, Wei SH, Hsueh KC, Lin WC (September 2007). "Endoscopic removal of foreign bodies in children". Kaohsiung J. Med. Sci. 23 (9): 447–52. doi:10.1016/S1607-551X(08)70052-4. PMID 17766213.
- ↑ "Battery Ingestion". Retrieved 2008-12-18.
- ↑ Yardeni D, Yardeni H, Coran AG, Golladay ES (July 2004). "Severe esophageal damage due to button battery ingestion: can it be prevented?". Pediatr. Surg. Int. 20 (7): 496–501. doi:10.1007/s00383-004-1223-6. PMID 15221361.