Knee
| Knee | |
|---|---|
 Right knee seen from the right side | |
| Details | |
| System | Musculoskeletal system |
| Nerve | Femoral, obturator, sciatic |
| Identifiers | |
| Latin | Articulatio genus |
| MeSH | A01.378.610.450 |
| TA | A01.1.00.036 |
| FMA | 24974 |
The knee joint joins the thigh with the leg and consists of two articulations: one between the femur and tibia (tibiofemoral joint), and one between the femur and patella (patellofemoral joint).[1] It is the largest joint in the human body.[2] The knee is a modified hinge joint, which permits flexion and extension as well as slight internal and external rotation. The knee joint is vulnerable to injury and to the development of osteoarthritis.
It is often termed a compound joint having tibiofemoral and patellofemoral components.[3][4] (The fibular collateral ligament is often considered with tibiofemoral components.)[5]
Structure



The knee is a modified hinge joint, a type of synovial joint, which is composed of three functional compartments: the patellofemoral articulation, consisting of the patella, or "kneecap", and the patellar groove on the front of the femur through which it slides; and the medial and lateral tibiofemoral articulations linking the femur, or thigh bone, with the tibia, the main bone of the lower leg.[6] The joint is bathed in synovial fluid which is contained inside the synovial membrane called the joint capsule. The posterolateral corner of the knee is an area that has recently been the subject of renewed scrutiny and research.
The knee is the largest joint and one of the most important joints in the body. It plays an essential role in movement related to carrying the body weight in horizontal (running and walking) and vertical (jumping) directions.
At birth, the kneecap is just formed from cartilage, and this will ossify (change to bone) between the ages of three and five years. Because it is the largest sesamoid bone in the human body, the ossification process takes significantly longer.[7]
Articular bodies
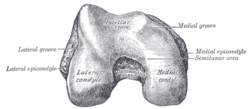
The articular bodies of the femur are its lateral and medial condyles. These diverge slightly distally and posteriorly, with the lateral condyle being wider in front than at the back while the medial condyle is of more constant width.[8] The radius of the condyles' curvature in the sagittal plane becomes smaller toward the back. This diminishing radius produces a series of involute midpoints (i.e. located on a spiral). The resulting series of transverse axes permit the sliding and rolling motion in the flexing knee while ensuring the collateral ligaments are sufficiently lax to permit the rotation associated with the curvature of the medial condyle about a vertical axis.[9]
The pair of tibial condyles are separated by the intercondylar eminence[8] composed of a lateral and a medial tubercle.[10]
The patella is inserted into the thin anterior wall of the joint capsule.[8] On its posterior surface is a lateral and a medial articular surface,[9] both of which communicate with the patellar surface which unites the two femoral condyles on the anterior side of the bone's distal end.[11]
Articular capsule
The articular capsule has a synovial and a fibrous membrane separated by fatty deposits. Anteriorly, the synovial membrane is attached on the margin of the cartilage both on the femur and the tibia, but on the femur, the suprapatellar bursa or recess extends the joint space proximally.[12] The suprapatellar bursa is prevented from being pinched during extension by the articularis genus muscle.[13] Behind, the synovial membrane is attached to the margins of the two femoral condyles which produces two extensions similar to the anterior recess. Between these two extensions, the synovial membrane passes in front of the two cruciate ligaments at the center of the joint, thus forming a pocket direct inward.[12]
Bursae
Numerous bursae surround the knee joint. The largest communicative bursa is the suprapatellar bursa described above. Four considerably smaller bursae are located on the back of the knee. Two non-communicative bursae are located in front of the patella and below the patellar tendon, and others are sometimes present. [12]
Cartilage
Cartilage is a thin, elastic tissue that protects the bone and makes certain that the joint surfaces can slide easily over each other. Cartilage ensures supple knee movement. There are two types of joint cartilage in the knees: fibrous cartilage (the meniscus) and hyaline cartilage. Fibrous cartilage has tensile strength and can resist pressure. Hyaline cartilage covers the surface along which the joints move. Cartilage will wear over the years. Cartilage has a very limited capacity for self-restoration. The newly formed tissue will generally consist of a large part of fibrous cartilage of lesser quality than the original hyaline cartilage. As a result, new cracks and tears will form in the cartilage over time.
Menisci
The articular disks of the knee-joint are called menisci because they only partly divide the joint space.[14] These two disks, the medial meniscus and the lateral meniscus, consist of connective tissue with extensive collagen fibers containing cartilage-like cells. Strong fibers run along the menisci from one attachment to the other, while weaker radial fibers are interlaced with the former. The menisci are flattened at the center of the knee joint, fused with the synovial membrane laterally, and can move over the tibial surface. [15][16]
The menisci serve to protect the ends of the bones from rubbing on each other and to effectively deepen the tibial sockets into which the femur attaches. They also play a role in shock absorption, and may be cracked, or torn, when the knee is forcefully rotated and/or bent.
Ligaments

The ligaments surrounding the knee joint offer stability by limiting movements and, together with the menisci and several bursae, protect the articular capsule.
Intracapsular
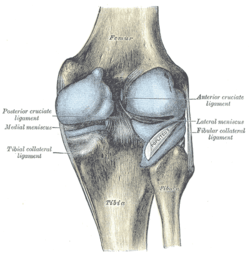
The knee is stabilized by a pair of cruciate ligaments. The anterior cruciate ligament (ACL) stretches from the lateral condyle of femur to the anterior intercondylar area. The ACL is critically important because it prevents the tibia from being pushed too far anterior relative to the femur. It is often torn during twisting or bending of the knee. The posterior cruciate ligament (PCL) stretches from medial condyle of femur to the posterior intercondylar area. Injury to this ligament is uncommon but can occur as a direct result of forced trauma to the ligament. This ligament prevents posterior displacement of the tibia relative to the femur.
The transverse ligament stretches from the lateral meniscus to the medial meniscus. It passes in front of the menisci. It is divided into several strips in 10% of cases.[15] The two menisci are attached to each other anteriorly by the ligament.[17] The posterior and anterior meniscofemoral ligaments stretch from the posterior horn of the lateral meniscus to the medial femoral condyle. They pass posteriorly behind the posterior cruciate ligament. The posterior meniscofemoral ligament is more commonly present (30%); both ligaments are present less often.[15] The meniscotibial ligaments (or "coronary") stretches from inferior edges of the mensici to the periphery of the tibial plateaus.
Extracapsular
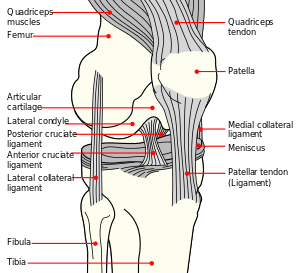
The patellar ligament connects the patella to the tuberosity of the tibia. It is also occasionally called the patellar tendon because there is no definite separation between the quadriceps tendon (which surrounds the patella) and the area connecting the patella to the tibia.[18] This very strong ligament helps give the patella its mechanical leverage[19] and also functions as a cap for the condyles of the femur. Laterally and medially to the patellar ligament the lateral and medial retinacula connect fibers from the vasti lateralis and medialis muscles to the tibia. Some fibers from the iliotibial tract radiate into the lateral retinaculum and the medial retinaculum receives some transverse fibers arising on the medial femoral epicondyle. [8]
The medial collateral ligament (MCL a.k.a. "tibial") stretches from the medial epicondyle of the femur to the medial tibial condyle. It is composed of three groups of fibers, one stretching between the two bones, and two fused with the medial meniscus. The MCL is partly covered by the pes anserinus and the tendon of the semimembranosus passes under it.[8] It protects the medial side of the knee from being bent open by a stress applied to the lateral side of the knee (a valgus force). The lateral collateral ligament (LCL a.k.a. "fibular") stretches from the lateral epicondyle of the femur to the head of fibula. It is separate from both the joint capsule and the lateral meniscus.[8] It protects the lateral side from an inside bending force (a varus force). The anterolateral ligament (ALL) is situated in front of the LCL.
Lastly, there are two ligaments on the dorsal side of the knee. The oblique popliteal ligament is a radiation of the tendon of the semimembranosus on the medial side, from where it is direct laterally and proximally. The arcuate popliteal ligament originates on the apex of the head of the fibula to stretch proximally, crosses the tendon of the popliteus muscle, and passes into the capsule.[8]
Muscles
The muscles responsible for the movement of the knee joint belong to either the anterior, medial or posterior compartment of the thigh. The extensors generally belong to the anterior compartment and the flexors to the posterior. The two exceptions to this is gracilis, a flexor, which belongs to the medial compartment and sartorius, a flexor, in the anterior compartment.
Extensors
Flexors
Posterior compartment
Medial compartment:
| Muscle | Origin | Insertion | Artery | Nerve | Action | Antagonist |
|---|---|---|---|---|---|---|
| Gracilis | Inferior pubic ramus[21] | Pes anserinus | Obturator artery | Anterior branch of obturator nerve[21] | Flexion and medial rotation of knee;[21] adduction of hip, flexion of hip, | |
Blood supply

The femoral artery and the popliteal artery help form the arterial network or plexus, surrounding the knee joint. There are six main branches: two superior genicular arteries, two inferior genicular arteries, the descending genicular artery and the recurrent branch of anterior tibial artery.
The medial genicular arteries penetrate the knee joint.
Function
| Extension 5-10° | Flexion 120-150° |
|---|---|
| Quadriceps (with some assistance from the Tensor fasciae latae) |
(In order of importance) Semimembranosus Semitendinosus Biceps femoris Gracilis Sartorius Popliteus Gastrocnemius |
| Internal rotation* 10° | External rotation* 30-40° |
| (In order of importance) Semimembranosus Semitendinosus Gracilis Sartorius Popliteus |
Biceps femoris |
| *(knee flexed 90°) | |
The knee permits flexion and extension about a virtual transverse axis, as well as a slight medial and lateral rotation about the axis of the lower leg in the flexed position. The knee joint is called "mobile" because the femur and lateral meniscus move[24] over the tibia during rotation, while the femur rolls and glides over both menisci during extension-flexion.[25]
The center of the transverse axis of the extension/flexion movements is located where both collateral ligaments and both cruciate ligaments intersect. This center moves upward and backward during flexion, while the distance between the center and the articular surfaces of the femur changes dynamically with the decreasing curvature of the femoral condyles. The total range of motion is dependent on several parameters such as soft-tissue restraints, active insufficiency, and hamstring tightness.[22]
Extended position
With the knee extended both the lateral and medial collateral ligaments, as well as the anterior part of the anterior cruciate ligament, are taut. During extension, the femoral condyles glide and roll into a position which causes the complete unfolding of the tibial collateral ligament. During the last 10° of extension, an obligatory terminal rotation is triggered in which the knee is rotated medially 5°. The final rotation is produced by a lateral rotation of the tibia in the non-weight-bearing leg, and by a medial rotation of the femur in the weight-bearing leg. This terminal rotation is made possible by the shape of the medial femoral condyle, assisted by contraction of the popliteus muscle and the iliotibial tract and is caused by the stretching of the anterior cruciate ligament. Both cruciate ligaments are slightly unwinded and both lateral ligaments become taut.[25]
Flexed position
In the flexed position, the collateral ligaments are relaxed while the cruciate ligaments are taut. Rotation is controlled by the twisted cruciate ligaments; the two ligaments get twisted around each other during medial rotation of the tibia — which reduces the amount of rotation possible — while they become unwound during lateral rotation of the tibia. Because of the oblique position of the cruciate ligaments at least a part of one of them is always tense and these ligaments control the joint as the collateral ligaments are relaxed. Furthermore, the dorsal fibers of the tibial collateral ligament become tensed during extreme medial rotation and the ligament also reduces the lateral rotation to 45-60°.[25]
Clinical significance
Knee pain is caused by trauma, misalignment, and degeneration as well as by conditions like arthritis.[26] The most common knee disorder is generally known as patellofemoral syndrome.The majority of minor cases of knee pain can be treated at home with rest and ice but more serious injuries do require surgical care.
One form of patellofemoral syndrome involves a tissue-related problem that creates pressure and irritation in the knee between the patella and the trochlea (patellar compression syndrome), which causes pain. The second major class of knee disorder involves a tear, slippage, or dislocation that impairs the structural ability of the knee to balance the leg (patellofemoral instability syndrome). Patellofemoral instability syndrome may cause either pain, a sense of poor balance, or both.[27]
Prepatellar bursitis also known as housemaid's knee is painful inflammation of the prepatellar bursa (a frontal knee bursa) often brought about by occupational activity such as a roofer.
Age also contributes to disorders of the knee. Particularly in older people, knee pain frequently arises due to osteoarthritis. In addition, weakening of tissues around the knee may contribute to the problem.[28] Patellofemoral instability may relate to hip abnormalities or to tightness of surrounding ligaments.[27]
Cartilage lesions can be caused by:
- Accidents (fractures)
- Injuries
- The removal of a meniscus
- Anterior cruciate ligament injury
- Posterior cruciate ligament injury
- Posterolateral corner injury
- Medial knee injuries
- Considerable strain on the knee.
Any kind of work during which the knees undergo heavy stress may also be detrimental to cartilage. This is especially the case in professions in which people frequently have to walk, lift, or squat. Other causes of pain may be excessive on, and wear off, the knees, in combination with such things as muscle weakness and overweight.
Common complaints:
- A painful, blocked, locked or swollen knee.
- Sufferers sometimes feel as if their knees are about to give way, or may feel uncertain about their movement.
Overall fitness and knee injury
Physical fitness is related integrally to the development of knee problems. The same activity such as climbing stairs may cause pain from patellofemoral compression for someone who is physically unfit, but not for someone else (or even for that person at a different time). Obesity is another major contributor to knee pain. For instance, a 30-year-old woman who weighed 120 lb at age 18 years, before her three pregnancies, and now weighs 285 lb, had added 660 lb of force across her patellofemoral joint with each step.[29]
Common injuries due to physical activity

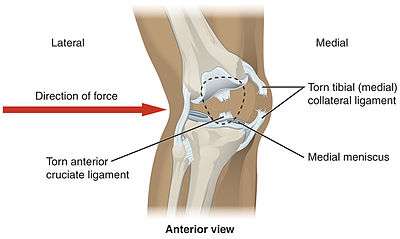
In sports that place great pressure on the knees, especially with twisting forces, it is common to tear one or more ligaments or cartilages. Some of the most common knee injuries are those to the medial side: Common genetic deficiencies can accelerate injuries and limit movement. A common Spanish term for individuals suffering from these characteristics is "Chaconist" (weak knee's). medial knee injuries.
Anterior cruciate ligament injury
The anterior cruciate ligament is the most commonly injured ligament of the knee. The injury is common during sports. Twisting of the knee is a common cause of over-stretching or tearing the ACL. When the ACL is injured a popping sound may be heard, and the leg may suddenly give out. Besides swelling and pain, walking may be painful and the knee will feel unstable. Minor tears of the anterior cruciate ligament may heal over time, but a torn ACL requires surgery. After surgery, recovery is prolonged and low impact exercises are recommended to strengthen the joint.[30]
Torn meniscus injury
The menisci act as shock absorbers and separate the two ends of bone in the knee joint. There are two menisci in the knee, the medial (inner) and the lateral (outer). When there is torn cartilage, it means that the meniscus has been injured. Meniscus tears occur during sports often when the knee is twisted. Menisci injury may be innocuous and one may be able to walk after a tear, but soon swelling and pain set in. Sometimes the knee will lock while bending. Pain often occurs when one squats. Small meniscus tears are treated conservatively but most large tears require surgery.[31]
Fractures

Knee fractures are rare but do occur, especially as a result of motor vehicle accidents. There is usually immediate pain; swelling and one may not be able to stand on the leg. The muscles go into spasm and even the slightest movements are painful. X-rays can easily confirm the injury and surgery depends on the degree of displacement and type of fracture.
Ruptured tendon
Tendons usually attach muscle to bone. In the knee the quadriceps and patellar tendon can sometimes tear. The injuries to these tendons occur when there is forceful contraction of the knee. If the tendon is completely torn, bending or extending the leg is impossible. A completely torn tendon requires surgery but a partially torn tendon can be treated with leg immobilization followed by physical therapy.
Overuse
Overuse injuries of the knee include tendonitis, bursitis, muscle strains and iliotibial band syndrome. These injuries often develop slowly over weeks or months. Activities that induce pain usually delay healing. Rest, ice and compression do help in most cases. Once the swelling has diminished, heat packs can increase blood supply and promote healing. Most overuse injuries subside with time but can flare up if the activities are quickly resumed.[32] Individuals may reduce the chances of overuse injuries by warming up prior to exercise, by limiting high impact activities and keep their weight under control.
Surgical interventions
Before the advent of arthroscopy and arthroscopic surgery, patients having surgery for a torn ACL required at least nine months of rehabilitation, having initially spent several weeks in a full-length plaster cast. With current techniques, such patients may be walking without crutches in two weeks, and playing some sports in a few months.
In addition to developing new surgical procedures, ongoing research is looking into underlying problems which may increase the likelihood of an athlete suffering a severe knee injury. These findings may lead to effective preventive measures, especially in female athletes, who have been shown to be especially vulnerable to ACL tears from relatively minor trauma.
Articular cartilage repair treatment :
- Arthroscopic debriment of the knee (arthroscopic lavage).
- Mosaïc-plasty.
- Microfracture (Ice-picking).
- Autologous Chondrocyte Implantation.
- Osteochondral Autograft and Allografts.
- PLC Reconstruction
Animal anatomy
In humans the knee refers to the joints between the femur, tibia and patella. In quadrupeds, particularly horses and ungulates the layman's term "knee" is commonly used to refer to the carpus. The joints between the femur, tibia and patella are known as the stifle in quadrupeds. In insects and other animals the term knee is used widely to refer to any ginglymus joint.
See also
- Arthrofibrosis
- Articular cartilage repair
- Autologous Chondrocyte Implantation
- Chondromalacia patellae
- Fibular collateral ligament
- Geniculum
- Genuflection
- Knee arthritis
- Knee Cartilage Replacement Therapy
- Knee examination
- Knee-capping
- Kneeling
- Knesetja
- Medial collateral ligament
- Partial knee replacement
- Posterolateral Knee Injuries
- Reflex hammer
Additional images
.ogv.jpg) Real-time MRI- Knee
Real-time MRI- Knee Knee MR
Knee MR Knee MR
Knee MR Knee X-ray
Knee X-ray Knee X-ray (Front)
Knee X-ray (Front) Cruciate ligaments
Cruciate ligaments Left knee-joint from behind, showing interior ligaments.
Left knee-joint from behind, showing interior ligaments.- Capsule of right knee-joint (distended). Lateral aspect.
 Anterior and lateral view of knee.
Anterior and lateral view of knee. Anterior view of knee.
Anterior view of knee.
Notes
- ↑ Chhajer, Bimal (2006). "Anatomy of Knee". Knee Pain. Fusion Books. pp. 10–1. ISBN 978-81-8419-181-3.
- ↑ Kulowski, Jacob (July 1932). "Flexion contracture of the knee". The Journal of Bone & Joint Surgery. 14 (3): 618–63. Republished as: Kulowski, J (2007). "Flexion contracture of the knee: The mechanics of the muscular contracture and the turnbuckle cast method of treatment; with a review of fifty-five cases. 1932". Clinical orthopaedics and related research. 464: 4–10. doi:10.1097/BLO.0b013e31815760ca (inactive 2015-05-08). PMID 17975372.
- ↑ Rytter, Søren; Egund, Niels; Jensen, Lilli; Bonde, Jens (2009). "Occupational kneeling and radiographic tibiofemoral and patellofemoral osteoarthritis". Journal of Occupational Medicine and Toxicology. 4: 19. doi:10.1186/1745-6673-4-19. PMC 2726153
 . PMID 19594940.
. PMID 19594940. - ↑ Gill, T. J.; Van De Velde, S. K.; Wing, D. W.; Oh, L. S.; Hosseini, A.; Li, G. (2009). "Tibiofemoral and Patellofemoral Kinematics After Reconstruction of an Isolated Posterior Cruciate Ligament Injury: In Vivo Analysis During Lunge". The American Journal of Sports Medicine. 37 (12): 2377–85. doi:10.1177/0363546509341829. PMC 3832057. PMID 19726621.
- ↑ Scott, Jacob; Lee, Ho; Barsoum, Wael; Van Den Bogert, Antonie J. (2007). "The effect of tibiofemoral loading on proximal tibiofibular joint motion". Journal of Anatomy. 211 (5): 647–53. doi:10.1111/j.1469-7580.2007.00803.x. PMC 2375777. PMID 17764523.
- ↑ Burgener (2002), p 390
- ↑ "Do babies have kneecaps?". HowStuffWorks.com.
- 1 2 3 4 5 6 7 Platzer (2004), p 206
- 1 2 Platzer (2004), pp 194-195
- ↑ Platzer (2004), p 202
- ↑ Platzer (2004), p 192
- 1 2 3 Platzer (2004), p 210
- ↑ Reider, B; Marshall, J. L.; Koslin, B; Ring, B; Girgis, F. G. (1981). "The anterior aspect of the knee joint". The Journal of bone and joint surgery. American volume. 63 (3): 351–6. PMID 7204430.
- ↑ Platzer (2004), p 26
- 1 2 3 Platzer (2004), p 208
- ↑ Gibbon, Anthony. "Knee Anatomy". North Yorkshire Orthopaedic Specialists. Retrieved 6 February 2013.
- ↑ Diab (1999), p 200
- ↑ MedicineNet.com, Definition of Patellar tendon
- ↑ Moore (2006), p 194
- 1 2 3 4 5 6 7 8 9 10 11 Gosling 2008, p. 273
- 1 2 3 Gosling et al. 2008, p. 266
- 1 2 Thieme Atlas of Anatomy (2006), pp 398-399
- ↑ Platzer (2004), p 252
- ↑ Thieme Atlas of Anatomy (2006), p 399
- 1 2 3 Platzer (2004), pp 212-213
- ↑ "Back of Knee Pain Causes
- 1 2 Afra R, Schepsis A (May 28, 2008). "Addressing patellofemoral pathology: Biomechanics and classification". The Journal of Musculoskeletal Medicine.
- ↑ Pill SG, Khoury LD, Chin GC, et al. (October 29, 2008). "MRI for evaluating knee pain in older patients: How useful is it?". The Journal of Musculoskeletal Medicine.
- ↑ Andrish JT (May 8, 2009). "Sports injuries in weekend warriors: 20 Clinical pearls". The Journal of Musculoskeletal Medicine. 26 (5).
- ↑ Knee pain and injuries About sports online portal. 2010-01-26
- ↑ Tandeter, Howard B. "Acute Knee Injuries: Use of Decision Rules for Selective Radiograph Ordering" 2010-01-26.
- ↑ Knee injuries and disorders MedLine Plus. 2010-01-26
References
- Burgener, Francis A.; Meyers, Steven P.; Tan, Raymond K. (2002). Differential Diagnosis in Magnetic Resonance Imaging. Thieme. ISBN 1-58890-085-1.
- Diab, Mohammad (1999). Lexicon of Orthopaedic Etymology. Taylor & Francis. ISBN 90-5702-597-3.
- Moore, Keith L.; Dalley, Arthur F.: Agur, A. M. R. (2006). Clinically Oriented Anatomy. Lippincott Williams & Wilkins. ISBN 0-7817-3639-0.
- Platzer, Werner (2004). Color Atlas of Human Anatomy, Vol. 1: Locomotor System (5th ed.). Thieme. pp. 206–213. ISBN 3-13-533305-1.
- "Definition of patellar tendon". MedicineNet.com. Retrieved 2008-12-11.
- Thieme Atlas of Anatomy: General Anatomy and Musculoskeletal System. Thieme. 2006. ISBN 1-58890-419-9.
External links
![]() Media related to Knee at Wikimedia Commons
Media related to Knee at Wikimedia Commons
| Look up knee in Wiktionary, the free dictionary. |