Shoulder girdle
| Shoulder girdle | |
|---|---|
 Human shoulder girdle | |
| Details | |
| Identifiers | |
| Latin | cingulum pectorale |
| TA | A01.1.00.020 |
| FMA | 23217 |
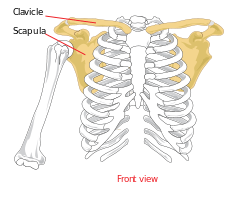
The shoulder girdle or pectoral girdle is the set of bones which connects the arm to the axial skeleton on each side. In humans it consists of the clavicle and scapula; in those species with three bones in the shoulder, it consists of the clavicle, scapula, and coracoid. Some mammalian species (such as the dog and the horse) have only the scapula.
The pectoral girdles are to the upper limbs as the pelvic girdle is to the lower limbs; the girdles are the parts of the appendicular skeleton that anchor the appendages to the axial skeleton.
In humans, the only true anatomical joints between the shoulder girdle and the axial skeleton are the sternoclavicular joints on each side. No anatomical joint exists between each scapula and the rib cage; instead the muscular connection or physiological joint between the two permits great mobility of the shoulder girdle compared to the compact pelvic girdle; because the upper limb is not usually involved in weight bearing, its stability has been sacrificed in exchange for greater mobility. In those species having only the scapula, no joint exists between the forelimb and the thorax, the only attachment being muscular.
Structure
Joints
The shoulder girdle is a complex of five joints that can be divided into two groups. Three of these joints are true anatomical joints while two are physiological ("false") joints.[explain 1] Within each group, the joints are mechanically linked so that both groups simultaneously contribute to the different movements of the shoulder to variable degrees. [1]
In the first group, the scapulohumeral or glenohumeral joint is the anatomical joint mechanically linked to the physiological subdeltoid or suprahumeral joint (the "second shoulder joint") so that movements in the latter results in movements in the former. In the second group, the scapulocostal or scapulothoracic joint is the important physiological joint that can not function without the two anatomical joints in the group, the acromioclavicular and sternoclavicular joints, i.e. they join both ends of the clavicle. [1]
Glenohumeral joint
The glenohumeral joint is the articulation between the head of the humerus and the glenoid cavity of the scapula. It is a ball and socket type of synovial joint with three rotatory and three translatory degree of freedom. The glenohumeral joint allows for adduction, abduction, medial and lateral rotation, flexion and extension of the arm.
Acromioclavicular joint
The acromioclavicular joint is the articulation between the acromion process of the scapula and the lateral end of the clavicle. It is a plane type of synovial joint. The acromion of the scapula rotates on the acromial end of the clavicle.
Sternoclavicular joint
The sternoclavicular joint is the articulation of the manubrium of the sternum and the first costal cartilage with the medial end of the clavicle. It is a saddle type of synovial joint but functions as a plane joint. The sternoclavicular joint accommodates a wide range of scapula movements and can be raised to a 60° angle.
Scapulocostal joint
The scapulocostal joint (also known as the scapulothoracic joint) is a physiological joint formed by an articulation of the anterior scapula and the posterior thoracic rib cage. It is musculotendinous in nature and is formed predominantly by the trapezius, rhomboids and serratus anterior muscles. The pectoralis minor also plays a role in its movements. The gliding movements at the scapulocostal joint are elevation, depression, retraction, protraction and superior and inferior rotation of the scapula. Disorders of the scapulocostal joint are not very common and usually restricted to snapping scapula.[2]
Suprahumeral joint
The suprahumeral joint (also known as the subacromial joint) is a physiological joint formed by an articulation of the coracoacromial ligament and the head of the humerus. It is formed by the gap between the humerus and the acromion process of the scapula. This space is filled mostly by the subacromial bursa and the tendon of supraspinatus. This joint plays a role during complex movements while the arm is fully flexed at the glenohumeral joint, such as changing a lightbulb, or painting a ceiling.
Movements
From its neutral position, the shoulder girdle can be rotated about an imaginary vertical axis at the medial end of the clavicle (the sternoclavicular joint). Throughout this movement the scapula is rotated around the chest wall so that it moves 15 centimetres (5.9 in) laterally and the glenoid cavity is rotated 40–45° in the horizontal plane. When the scapula is moved medially it lies in a frontal plane with the glenoid cavity facing directly laterally. At this position, the lateral end of the clavicle is rotated posteriorly so that the angle at the acromioclavicular joint opens up slightly. When the scapula is moved laterally it lies in a sagittal plane with the glenoid cavity facing anteriorly. At this position, the lateral end of the clavicle is rotated anteriorly so that the clavicle lies in a frontal plane. While this slightly closes the angle between the clavicle and the scapula, it also widens the shoulder. [3]
The scapula can be elevated and depressed from the neutral position to a total range of 10 to 12 centimetres (3.9 to 4.7 in); at its most elevated position the scapula is always tilted so that the glenoid cavity is facing superiorly. During this tilting, the scapula rotates to a maximum angle of 60° about an axis passing perpendicularly through the bone slightly below the spine; this causes the inferior angle to move 10 to 12 centimetres (3.9 to 4.7 in) and the lateral angle 5 to 6 centimetres (2.0 to 2.4 in). [3]
Exercises
[The anatomical mechanism that allows for all upper arm and shoulder movement is the shoulder girdle.[4] The shoulder girdle consists of five muscles that attach to the clavicle and scapula and allow for the motion of the sternoclavicular joint (connection between sternum and clavicle) and acromioclavicular joint (connection between clavicle and scapula).[5] The five muscles that comprise the function of the shoulder girdle are the trapezius muscle (upper, middle, and lower), levator scapulae muscle, rhomboid muscles (major and minor), serratus anterior muscle, and pectoralis minor muscle.[6]]
Strengthening the shoulder girdle
- Exercise 1
An exercise that promotes the strengthening of the muscles that move the shoulder girdle is barbell behind neck presses.[7] The exercise requires grasping the barbell with an overhand grip from a rack or from the floor and holding behind the neck in standing position. The first movement includes pressing bar upwards until arms are fully raised, this movement is an upward rotation of the scapula [8] which strengthens the upper trapezius, lower trapezius, and serratus anterior which aids in scapular stabilization.[9] The second movement is bringing the bar back down behind neck; this movement is a downward rotation of the scapula which strengthens the rhomboid major muscle, rhomboid minor muscle, levator scapulae, and pectoralis minor muscle <refHamilton=newyork2008/>. An alternative for this exercise is performing it while sitting in a chair with adequate back support.
- Exercise 2
An additional exercise that strengthens the shoulder girdle muscles is barbell shrugs which can also be known as shoulder shrug.[10] The exercise requires holding the barbell with overhand grip while in standing position. The first movement is raising the shoulders in a shrugging motion, this movement is elevation of the scapula <refHamilton=newyork2008/> which strengthens the upper trapezius, levator scapulae, rhomboids major, and rhomboids minor <refLippert=philadelphia2011/>. The second movement is lowering the shoulders below the regular level of shoulders’ resting point; this movement is depression of the scapula <refHamilton=newyork2008/> which strengthens the lower trapezius, and pectoralis minor <refLippert=philadelphia2011/>. An alternative for this exercise is sitting in a chair though performing all previously described shoulder motions. Another alternative is utilizing dumbbell weights and holding with thumbs facing forward.
- Exercise 3
An additional exercise that strengthens the shoulder girdle is barbell bent-over rows.[11] The exercise requires bending at hips and bringing torso forward. For this exercise, the back must be kept straight while holding the barbell with a wide overhand grip and bending the knees slightly. The first movement is bringing the bar up towards chest; this movement is retraction of the scapulae <refLippert=philadelphia2011/> which strengthens the middle trapezius, rhomboids major, and rhomboids minor muscle <refHamilton=newyork2008/>. The second movement is lowering the bar which is protraction of the scapulae <refLippert=philadelphia2011/> and strengthens the serratus anterior and pectoralis minor <refHamilton=newyork2008/>. An alternative for this exercise includes holding dumbbell weights with thumbs facing forward and following same motion. Another alternative is performing the exercise while seated in a chair and using dumbbell weights.
- Exercise 4
Another exercise that promotes strengthening of the shoulder girdle is dumbbell shoulder extensions. The exercise requires keeping back straight, and holding dumbbell weights at sides with palms facing back in preparation. The first movement is raising the weights while keeping arms straight and then bringing them back down; this movement is upward tilt of the scapula which strengthens the pectoralis minor <refLippert=philadelphia2011/>. Alternatives for the exercise include sitting in a chair or laying prone on an elevated surface though keeping back straight and executing same shoulder/arm motion.
Shoulder injury prevention
Common injuries
Shoulders are a common place for tissue injuries, especially if the person plays overhead sports such as tennis, volleyball, baseball, swimming, etc. According to Bahr’s major injury related statistics, shoulder dislocations or subluxations account for 4% of injuries in adults ages 20–30 and 20% of shoulder injuries are fractures.[12] Damage to the shoulder and adjacent features can fluctuate in severity depending on the person’s age, sport, position, recurring shoulder dysfunction, and many other factors. Some other common shoulder injuries are fractures to any shoulder girdle bones i.e. clavicle, ligamentous sprains such as AC joint or GH ligaments, rotator cuff injuries, different labral tears, and other acute or chronic conditions related to shoulder anatomy. In order to help limit or decrease the severity of an injury, proper maintenance and conditioning should take place. Proper warm ups, strengthening of the shoulder complex, and lifestyle choices can help bring positive lifelong use of the shoulders.
Conditioning/warm-ups
Conditioning of the shoulder area involves full body exercises through a full range of motion. Exercises that are light to moderate activity over a 30-60 minute time period should increase cardiac output, which in-turn helps carry more oxygen saturated blood throughout the body. Regular running or an upper body ergometer are examples of full body exercise to increase cardiovascular endurance for proper conditioning. The more blood that the heart can pump throughout the body helps endurance performance by supplying the body with more nutrients and oxygen for a prolonged period of time.[13] In addition to conditioning the heart; a good dynamic warm-up, particular to a sport, should be in place to help prevent shoulder injury. Dynamic warm ups for upper and lower body can be considered a form of conditioning. The athlete can stretch and perform small movements in multiple directions to increase neurovascular response which satisfies dynamic warm ups. The increase in blood flow and neurological feedback will help with physiological and mechanical components for sport performance. This also helps with the exchange of oxygen from the blood to the tissues and synapses of the neurons happening quicker which leads to enhanced performance.[14]
Strengthening
Shoulder Girdle strengthening is a preventative procedure to help minimize tissue damage or other injuries while completing complex progressions in sports. Strengthening of the shoulder area can done by exercising specific muscle groups which are as follow. The positioners of the shoulder are the rotator cuff muscles: supraspinatus, infraspinatus, teres minor, and subscapularis. Propellers are major movers to create force with the arms, which include larger muscles: pectoralis major/minor, latissimus dorsi, and trapezius. The stabilizers of the shoulder are the deltoid group. Several other muscles should not be forgotten that assist with control of scapula thoracic rhythm: rhomboid muscles, serratus posteriors, levator scapulae muscle, and others smaller muscles.[15] A key way to prevent shoulder injury is making sure to do slow and in control stretches and exercises in proper form with proper progression. In any sporting activity proper progression should include strengthening below 90 degrees, then progressing into a 90 degree range, and then full overhead exercises.[16] Specific progression exercises should target rotator cuff muscles and other muscles that attach to the shoulder girdle. Many individuals at gyms are injured because of incorrect equipment use. An experienced professional should assist with program development, progression, and implementation in injury prevention such as a certified personal trainer. If a minor shoulder injury does occur and isn’t severe, these measures can be taken to activate and recuperate the muscles: light stretching, light weightlifting, warm or cold packs as needed, and therapeutic message. Each sport has a different shoulder movement mechanics, and when executed correctly it will put less strain on the shoulder which in-turn preserves the shoulder longer.
Shoulder girdle pain
Shoulder girdle pain can be acute or chronic and be due to a number of causes. Inflammation or injury of associated tendons, bone, muscles, nerves, ligaments, and cartilage can all cause pain. Also past injury compensation, and stress can result in complicated shoulder pain.[17]
Trigger points
The shoulder girdle is a complicated area and pinpointing the source of pain can be very difficult. Figures 1 and 2 show the complexity of the shoulder girdle and the muscles included. The simplest of injuries can yield very difficult issues, because the body will always try to accommodate the weak points in movement. A distinction needs to be made between referred pain and the actual origin of pain. To help with treatment a therapist has to assess the trigger points. Trigger points are often reported as a regional, persistent pain that usually results in a decreased range of motion of the muscle in question.[18] Posterior trigger points of the shoulder girdle are located on the posterior deltoid, levator scapulae, the upper/ middle trapezius, infraspinatus, teres minor, subscapularis, latissimus dorsi and the triceps brachii, serratus anterior. Trigger points on the anterior side are located on the infraspinatus, anterior deltoid, scalene, suprapinatus, pectoralis major, pectoralis minor, biceps brachii, coracobrachialis, sternalis, subclavian, and the latissimus dorsi. Some trigger points are repetitive when it comes to pain felt both anteriorly and posteriorly that is due to referred pain. These trigger points can refer pain to the entire arm. From the back of shoulder up the back of the neck, the front of the shoulder, down the arm, and can even be felt in the wrist and hands. For example, referred pain from other areas like the cervical area can be felt in the shoulder girdle. Referred pain is due to nerves passing through the shoulder down the arm allowing pain to be felt away from the origin.
Taping
Taping can also help relieve pain in the shoulder. According to the textbook “Essentials of athletic injury management” by prentice and Arnheim, Athletic tape helps to alleviate pain by increasing circulation to affected area, provide support, provides a means for stabilizing the arm, and allows for pressure reduction.[19] When pain is cause from it being in a constant raise position. A technique where tape is applied to drop the shoulder can be used to get rid of the pain and strain by adding more space in the joint. For example, for the acromioclavicular joint taping can be applied to relieve pain in the top of the shoulder from a collision or as a result of the joint becoming separated because of damage to ligament. The way the shoulder is positioned can cause pain and retracting the shoulder by tapping can relieve the pain. See figure 3 for an illustration on shoulder tapping.
Corticosteroids
Corticosteroids may be used in extreme circumstances to decrease pain and swelling to an affected area. Corticosteroid are typically given orally or in an injection form. Once injections are given pain is usually relieved for several weeks at a time. See figure 4 for and illustration on corticosteroid injections orally, they have even shorter lasting effects. They typically last for about 3 weeks. According to the journal article “Shoulder pain” corticosteroids only reduce pain for a short term.[20] They are only a temporary solution to the problem. Because the corticosteroid injection is not a cure and at some point the symptoms are going to return. This injection should be a last resort but is often used with a combination of physical therapy and rehab to reduce the pain during that time as well as strengthen the area. Corticosteroid injection can only be used minutely and is recommended not to use these injections more than 3 times in a years’ time.
Therapy
Physical therapy and rehab therapy is also a great method to relieve pain and promote healing. According to Peter Ronai’s journal “Exercise Modifications and Strategies to Enhance Shoulder Function” appropriate training strategies for promoting shoulder stability and enhanced function can relieve shoulder pain and dysfunction.[21] A patient who demonstrates shoulder exercises and go through a series of massages to manipulate and strengthen the shoulder. It’s of great importance to maintain mobility in the shoulder. Because when you don’t use the shoulder for periods of time you can make it worse and the muscles start to waste away. Exercising the area may be painful but under a professional you will be given exercises that will be beneficial and not damage the shoulder any further.
Other animals
The shoulder girdle demonstrates an enormous variation in amniotes (animals adapted to a terrestrial life), both among extant species and along evolutionary lines, and determining homologies for individual pectoral elements is difficult. Except for the sternum, these elements were, however, present in early bony fishes before there were even limbs. In digitless tetrapods the cleithrum, clavicle, and interclavicle are dermal and linked to the caudal part of the head while the humerus articulates with a small scapulocoracoid bone. As the first digits appeared, the pectoral structure lost its direct connection to the head skeleton while the scapulocoracoid grew more prominent and started to face laterally. In more derived tetrapods the dermal part of the girdle was gradually reduced and the scapulocoracoid split into a dorsal scapula and a ventral coracoid. [22]
In dinosaurs
In dinosaurs the main bones of the pectoral girdle were the scapula (shoulder blade) and the coracoid, both of which directly articulated with the clavicle. The clavicle was present in saurischian dinosaurs but largely absent in ornithischian dinosaurs. The place on the scapula where it articulated with the humerus (upper bone of the forelimb) is the called the glenoid. The scapula served as the attachment site for a dinosaur's back and forelimb muscles.
In primates
Chimpanzees are far better adapted to brachiation than modern humans. Their clavicles possess a cranially oriented twist on the acromial end, conducive to better force transfer through it - a very important function in arboreal locomotion. Chimpanzee scapulas also possess a considerably larger supraspinous fossa, allowing for a larger supraspinatus muscle. Through the process of evolution, humans have lost the Atlantoclavicularis muscle, originating on the atlas of the vertebral column, and inserting onto the acromial clavicle. This muscle acts to elevate the clavicle.[23]
See also
Notes
References
- 1 2 Kapandji 1982, p. 20
- ↑ Arend CF. Ultrasound of the Shoulder. Master Medical Books, 2013. Free section on snapping scapula available at ShoulderUS.com
- 1 2 Kapandji 1982, p. 40
- ↑ Moezy, A., Sepehrifar, S., Dodaran, M. S. (2014). The effects of scapular stabilization based exercise therapy on pain, posture, flexibility and shoulder mobility in patients with shoulder impingement syndrome: a controlled randomized clinical trial. Medical Journal of the Islamic Republic of Iran (MJIRI) Iran University of Medical Sciences, (Vol 28.87), 1-15.
- ↑ Saladin, K. (2011). Human Anatomy (3rd ed.). New York, NY: McGraw-Hill Companies.
- ↑ Lippert, L. (2011). Clinical Kinesiology and Anatomy (5th ed.). Philadelphia, PA: F. A. Davis Company.
- ↑ Barbell Behind Neck Presses. http://www.exrx.net/WeightExercises/DeltoidAnterior/BBBehindNeckPress.html.
- ↑ Hamilton, N. Ph.D., Weimer, W. Ph.D., & Luttgens, K. Ph.D. (2008). Kinesiology: Scientific Basis of Human Motion (11th ed.). New York, NY: McGraw-Hill Companies.
- ↑ . Smith, J. MD, Dahm, D. L. MD, Kaufman, K. R. Ph.D., Boon, A. J. MD, Laskowski, E. R. MD, Kotajarvi, B. R. PT, Jacofsky, D. J. MD (2006). Electromyographic Activity in the Immobilized Shoulder Girdle Musculature During Scapulothoracic Exercises. American Congress of Rehabilitation Medicine and the American Academy of Physical Medicine and Rehabilitation, (Vol 87), 923-927.
- ↑ Dumbbell Shrug. http://www.exrx.net/WeightExercises/TrapeziusUpper/DBShrug.html.
- ↑ Barbbell Bent-Over Row. http://www.exrx.net/WeightExercises/BackGeneral/BBBentOverRow.html.
- ↑ Bahr, R. (2012). IOC Manual of Sports Injuries : An Illustrated Guide to the Management of Injuries in Physical Activity. Somerset, NJ, USA: John Wiley & Sons
- ↑ Kjaer, M., Krogsgaard, M., & Magnusson, P. (Eds.). (2008). Textbook of Sports Medicine : Basic Science and Clinical Aspects of Sports Injury and Physical Activity. Chichester, GBR: John Wiley & Sons
- ↑ Moynes, D. R. (1983). Clinics in sports medicine: Prevention of Injury to the Shoulder Through Exercises and Therapy
- ↑ Davis, G. J., Durall, C. J., Manske, R. C. (2001). Avoiding Shoulder Injury From Resistance Training. National Strength & Conditioning Association. Vol. 23. Num. 5. Pgs. 10-18
- ↑ Houglan, P. A. (2010). Therapeutic Exercises for Musculoskeletal Injuries, Third edition. Champaign, IL, USA: Human Kinetics
- ↑ Mitchell, Caroline; et al. (2005). "Shoulder Pain: Diagnosis and Management in Primary Care". BMJ. 331 (7525): 1124–1128. doi:10.1136/bmj.331.7525.1124.
- ↑ Alvarez, David J., Rockwell, Pamala Trigger Points: Diagnosis and Management. Am Fam Physician. 2002 Feb 15;65(4):653-661.http://www.aafp.org/afp/2002/0215/p653.html
- ↑ Prentice, W., & Arnheim, D. (2012). "Essentials of athletic injury management" (9th ed.). Boston: McGraw-Hill
- ↑ Murphy, Richard J; Carr, Andrew J (2010). "Shoulder Pain". Clinical Evidence. 2010: 1107. PMC 3217726
 . PMID 21418673.
. PMID 21418673. - ↑ Ronai, Peter. "Exercise Modifications and Strategies to Enhance Shoulder Function." Strength and Conditioning Journal 27.4 (2005): 36-45. http://www.nsca.com/education/articles/exercise-modifications-to-enhance-shoulder-function
- ↑ Vickaryous & Hall 2006, Introduction, see also Fig. 1
- ↑ Bramble, Dennis; Lieberman, Daniel (23 September 2004). "Endurance running and the evolution of Homo". Nature. 432: 345–352. doi:10.1038/nature03052. PMID 15549097. Retrieved 14 November 2014.
References
- Kapandji, Ibrahim Adalbert (1982). The Physiology of the Joints: Volume One Upper Limb (5th ed.). New York: Churchill Livingstone.
- Roy, André (June 2009). "Rotator Cuff Disease Clinical Presentation". MedScape. Retrieved July 2011. Check date values in:
|access-date=(help) - Vickaryous, Matthew K; Hall, Brian K (March 2006). "Homology of the reptilian coracoid and a reappraisal of the evolution and development of the amniote pectoral apparatus". Journal of Anatomy. 208 (3): 263–285. doi:10.1111/j.1469-7580.2006.00542.x.