Prognathism
| Prognathism | |
|---|---|
 | |
| Classification and external resources | |
| Specialty | orthodontics |
| ICD-10 | M26.10 |
| ICD-9-CM | 524.10 |
| DiseasesDB | 29354 |
| MedlinePlus | 003026 |
| MeSH | D011378 |
Prognathism is the positional relationship of the mandible and/or maxilla to the skeletal base where either of the jaws protrudes beyond a predetermined imaginary line in the coronal plane of the skull. In general dentistry, oral and maxillofacial surgery and orthodontics, this is assessed clinically or radiographically (cephalometrics). The word "prognathism" derives from Greek pro (forward) and γνάθος gnathos (jaw). One or more types of prognathism may result in the common condition of malocclusion, in which an individual's top teeth and lower teeth do not align properly.
Presentation
Prognathism in humans can be due to normal variation among phenotypes. In human populations where prognathism is not the norm, it may be a malformation, the result of injury, a disease state or a hereditary condition.[1] Prognathism is considered a disorder only if it affects mastication, speech or social function as a byproduct of severely affected aesthetics of the face.
Clinical determinants include soft tissue analysis where the clinician assesses nasolabial angle, the relationship of the soft tissue portion of the chin to the nose, and the relationship between the upper and lower lips; also used is dental arch relationship assessment such as Angle's classification.
Cephalometric analysis is the most accurate way of determining all types of prognathism, as it includes assessments of skeletal base, occlusal plane angulation, facial height, soft tissue assessment and anterior dental angulation. Various calculations and assessments of the information in a cephalometric radiograph allow the clinician to objectively determine dental and skeletal relationships and determine a treatment plan.
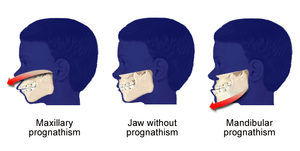
Maxillary prognathism is a protrusion of the maxilla, and is a common feature in Sub Saharan Africans. Prognathism is less prevalent in East Asians and Caucasians. It is not to be confused with micrognathism, although combinations of both may be found. It affects the middle third of the face, causing it to jut out, thereby increasing the facial area, similar in phenotype of archaic hominids and apes. Mandibular prognathism is a protrusion of the mandible, affecting the lower third of the face. Alveolar prognathism is a protrusion of that portion of the maxilla where the teeth are located, in the dental lining of the upper jaw. Prognathism can also be used to describe ways that the maxillary and mandibular dental arches relate to one another, including malocclusion (where the upper and lower teeth do not align). When there is maxillary and/or alveolar prognathism which causes an alignment of the maxillary incisors significantly anterior to the lower teeth, the condition is called an overjet. When the reverse is the case, and the lower jaw extends forward beyond the upper, the condition is referred to as retrognathia (reverse overjet).
Classification
Alveolar prognathism

Not all alveolar prognathism is anomalous, and significant differences can be observed among different ethnic groups.[2]
Harmful habits such as thumb sucking or tongue thrusting can result in or exaggerate an alveolar prognathism, causing teeth to misalign. Functional appliances can be used in growing children to help modify bad habits and neuro-muscular function, with the aim of correcting this condition.
Alveolar prognathism can also easily be corrected with fixed orthodontic therapy. However, relapse is quite common, unless the cause is removed or a long-term retention is used.
Maxillary prognathism
In disease states, maxillary prognathism is associated with Cornelia de Lange Syndrome;[3] however, so-called false maxillary prognathism, or more accurately, retrognathism, where there is a lack of growth of the mandible, is by far a more common condition.
Prognathism, if not extremely severe, can be treated in growing patients with orthodontic functional or orthopaedic appliances. In adult patients this condition can be corrected by means of a combined surgical/orthodontic treatment, where most of the time a mandibular advancement is performed. The same can be said for mandibular prognathism.
Mandibular prognathism (progenism)

Pathologic mandibular prognathism is a potentially disfiguring genetic disorder where the lower jaw outgrows the upper, resulting in an extended chin. It is sometimes a result of acromegaly.
This condition is colloquially known as lantern jaw, as well as Habsburg jaw, Habsburg lip or Austrian Lip (see House of Habsburg) due to its prevalence in that bloodline.[4] The trait is easily traceable in portraits of Habsburg family members.[5] This has provided tools for people interested in studying genetics and pedigree analysis. Most instances are considered polygenetic.[6]
It is alleged to have been derived through a female from the princely Polish family of Piast, its Mazovian branch. The deformation of lips is clearly visible on tomb sculptures of Mazovian Piasts in the St. John's Cathedral in Warsaw. However this may be, there exists evidence that the trait is longstanding. It is perhaps first observed in Vlad Dracula (1431–1476/77) and Maximilian I (1459–1519).
Traits such as these that were common to royal families are believed to have been passed on and exaggerated over time through royal intermarriage which caused acute inbreeding. Due to the large amount of politically motivated intermarriage among Habsburgs, the dynasty was virtually unparalleled in the degree of its inbreeding. Charles II of Spain is said to have had the most pronounced case of the Habsburg jaw on record. His jaw was so deformed that he was unable to chew.
Many dog breeds have underbite, particularly those with short faces, like shih tzus and boxers. This may be due, as in the case of bulldogs, to a slower growing maxilla in relation to the mandible.
Treatment

The surgery required has led, in some cases, to identity crisis in patients, whereby the new facial structure has a negative impact mentally of how the patient perceives themselves.
The most common treatment for mandibular prognathism is a combination of orthodontics and orthognathic surgery. The orthodontics can involve braces, removal of teeth, or a mouthguard.
History
Prognathism is well recorded as a trait of several historic individuals. The most famous case is that of the House of Habsburg, among whom mandibular prognathism was a family trait; indeed, the condition is frequently called "Habsburg Jaw" as a result of its centuries-long association with the family. Among the Habsburgs, the most prominent case of mandibular prognathism is that of Charles II of Spain, who had prognathism so pronounced he could neither speak clearly nor chew as a result of generations of politically motivated inbreeding.
See also
- Biological anthropology
- Charles II of Spain#Early life
- Chin
- Craniofacial anthropometry
- Forensics
- Homo erectus
- Hominid dental morphology evolution
- Physical anthropology
References
- ↑ MedlinePlus Medical Encyclopedia: Prognathism
- ↑ Vioarsdóttir US, O'Higgins P, Stringer C (2002). "A geometric morphometric study of regional differences in the ontogeny of the modern human facial skeleton". J. Anat. 201 (3): 211–29. doi:10.1046/j.1469-7580.2002.00092.x. PMC 1570912
 . PMID 12363273.
. PMID 12363273. - ↑ de Lange syndrome definition - Medical Dictionary definitions of popular medical terms easily defined on MedTerms
- ↑ Online Mendelian Inheritance in Man (OMIM) PROGNATHISM, MANDIBULAR -176700
- ↑ Chudley, Albert E. (1998). "Genetic landmarks through philately – the Habsburg jaw". Clinical Genetics. 54 (4): 283–4. doi:10.1034/j.1399-0004.1998.5440404.x. PMID 9831338.
- ↑ Wolff G, Wienker TF, Sander H (1993). "On the genetics of mandibular prognathism: analysis of large European noble families". J. Med. Genet. 30 (2): 112–116. doi:10.1136/jmg.30.2.112. PMC 1016265. PMID 8445614.
External links
-
 The dictionary definition of prognathism at Wiktionary
The dictionary definition of prognathism at Wiktionary