U wave
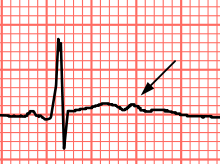
The U wave is a wave on an electrocardiogram that is not always seen. It is typically small, and, by definition, follows the T wave. U waves are thought to represent repolarization of the Purkinje fibers.[1] In the opinion of V. Gorshkov-Cantacuzene "the U wave is the momentum carried by the blood in the coronary arteries and blood vessels".[2][3][4] The resistivity of stationary blood is expressed as (Ht)=|Ht · (1+ αHt) , where α – is a coefficient, Ht – is the hematocrit; at that time, as during acceleration of the blood flow occurs a sharp decrease in the longitudinal resistance with small relaxation times. On the other hand, there are a number of factors affecting the resistivity of blood. Erythrocyte aggregation occurs at low shear rates and this leads to the conclusion that all vessels (with the exception of large venous) the effect of aggregation is irrelevant. In a blood vessel includes the near-wall layer of plasma (referred to as lubricant), whose size strictly depends on the Reynolds criterion and the shear rate. Given that the thickness of this layer in all blood vessels (except capillaries) is less than 5 microns, and the resistivity of the plasma is two times less than in blood, according to the scheme of parallel inserting is easy to estimate that the contribution of this layer to the resistivity is negligible. By reducing the speed of blood flow profiles of the dependence of Ht on the radius of the vessel becomes more elongated. However, at normal values of Ht, the effect is also insignificant contribution. With enough shear rates the red blood cells susceptible to deformation. The contribution of this phenomenon is difficult to assess, because it is present in the background of all the above effects. However, even the sum of all these factors has little effect on the resistivity of blood.
From this it follows that at the time of ejection of blood from the left ventricular part of the pulse is carried away, because there is no electrical resistivity of blood, which gradually increases high up in the coronary arteries and blood vessels. Thus, we can conclude that the U wave is the momentum carried by the blood in the coronary arteries and blood vessels. Further, it is possible to taking this momentum back to Purkinje fibers along the vessels of the myocardium. This idea is also proved by the fact that hypertrophy of the left ventricle, myocardial ischemia, coronary insufficiency have momentum there is no possibility to move on to the Purkinje fibers, therefore, the ECG recorded negative U wave.
Interpretation
According to many studies U wave often fails to register in all leads except the V6, while most often in V2 and V3 with heart rate less than 96 beats per minute. Its amplitude often is 0.1–0.33 mV. Particularly difficult is the allocation of the boundaries of the U wave on the background of the T wave and R wave, which may partial or complete (in the case of T wave) the merger. It is shown that higher values of heart rate or hypocalcemia U wave are superimposed on the T wave and in tachycardia — merges with the R wave of the next cardiac cycle.
Prominent U waves are most often seen in hypokalemia but may be present in hypercalcemia, thyrotoxicosis, or exposure to digitalis, epinephrine, and Class 1A and 3 antiarrhythmics, as well as in congenital long QT syndrome, and in the setting of intracranial hemorrhage.
An inverted U wave may represent myocardial ischemia (and especially appears to have a high positive predictive accuracy for left anterior descending coronary artery disease[5] ) or left ventricular volume overload.[6]
A U-wave can sometimes be seen in normal younger, athletic individuals.[7]
References
- ↑ Pérez Riera AR, Ferreira C, Filho CF, et al. (2008). "The enigmatic sixth wave of the electrocardiogram: the U wave". Cardiol J. 15 (5): 408–21. PMID 18810715.
- ↑ V, Gorshkov-Cantacuzene (2016). "TO THE QESTION OF THE ETHIOLOGY AND CLINICAL SIGNIFICANCE OF THE U WAWE OF THE ECG.". Bulletin of Science and Practice. 10(11): 130–133. doi:10.5281/zenodo.161068. ISSN 2414-2948.
- ↑ V A, Gorshkov-Cantacuzene (2015). "The clinical significance of the ECG U wave". Abstracts of XV Congress of "Heart Failure - 2015": 80.
- ↑ V A, Gorshkov-Cantacuzene. "Etiology and clinical significance of the ECG U wave". Proceedings of the Russian National Congress of Cardiologists. Cardiology 2016: Challenges and Solutions, Section: Fundamental Research: 520–521.
- ↑ Gerson MC, Phillips JF, Morris SN, McHenry PL (1979). "Exercise-induced U-wave inversion as a marker of stenosis of the left anterior descending coronary artery". Circulation. 60: 1014–1020. doi:10.1161/01.CIR.60.5.1014. PMID 487534.
- ↑ Conrath C, Opthof T (2005). "The patient U wave". Cardiovasc Res. 67 (2): 184–6. doi:10.1016/j.cardiores.2005.05.027. PMID 15979057.
- ↑ EKG-boken Ylva Lind, Lars Lind, Liber, 2011