Vulvar cancer
| Vulvar cancer | |
|---|---|
| Classification and external resources | |
| ICD-9-CM | 4 184. 4 |
Vulvar cancer is a malignant, invasive growth in the vulva, or the outer portion of the female genitals. The disease accounts for only 0.6% of cancer diagnoses[1] but 5% of gynecologic cancers in the United States.[2] The labia majora are the most common site involved representing about 50% of all cases, followed by the labia minora.[3] The clitoris and Bartholin glands may rarely be involved.[4] Vulvar cancer is separate from vulvar intraepithelial neoplasia (VIN), a superficial lesion of the epithelium that has not invaded the basement membrane—or a pre-cancer.[5] VIN may progress to carcinoma-in-situ and, eventually, squamous cell cancer.
According to the American Cancer Society, in 2014, there were about 4,850 new cases of vulvar cancer and 1,030 deaths from the disease.[6] In the United States, five-year survival rates for vulvar cancer are around 70%.[7]
Types
Squamous cell carcinoma
Most vulvar cancer (approximately 90%)[8] is squamous cell carcinoma, which originates from epidermal squamous cells, the most common type of skin cell. Carcinoma-in-situ is a precursor lesion of squamous cell cancer that does not invade through the basement membrane. While this type of lesion is more common with older age, young women with risk factors may also be affected. In the elderly, complications may occur due to the presence of other medical conditions.
Squamous lesions tend to arise in a single site and occur most commonly in the vestibule.[9] They grow by local extension and spread via the local lymph system. The lymphatics of the labia drain to the upper vulva and mons, then to both superficial and deep inguinal and femoral lymph nodes. The last deep femoral node is called the Cloquet’s node.[9] Spread beyond this node reaches the lymph nodes of the pelvis. The tumor may also invade nearby organs such as the vagina, urethra, and rectum and spread via their lymphatics.
A verrucous carcinoma of the vulva is a rare subtype of squamous cell cancer and tends to appear as a slowly growing wart. Verrucous vulvar cancers tend to have good overall prognoses.[10]
Melanoma
Melanoma is the second most common type of vulvar cancer and causes 8–10% of vulvar cancer cases.[9] These lesions arise from melanocytes, the cells that give skin color and are most common in Caucasian women 50–80 years old.[11] Melanoma of the vulva behaves like melanoma in any other location and may affect a much younger population.
There are three distinct types of vulvar melanoma: superficial spreading, nodular, and acral lentigous melanoma. Vulvar melanomas are unique in that they are microstaged with the Chung, Clark and/or Breslow systems, which specify stage and tumor depth of invasion. In general, they come with a high risk of metastasis and carry a poor overall prognosis.[9]
Basal cell carcinoma
Basal cell carcinoma makes up about 1–2% of vulvar cancer. These tend to be slow-growing lesions on the labia majora but can occur anywhere on the vulva. Their behavior is similar to basal cell cancers in other locations. They often grow locally and have low risk for deep invasion or metastasis.
Treatment involves excision, but these lesions have a tendency to recur if not completely removed.[12]
Bartholin gland carcinoma
The Bartholin gland is a rare malignancy and usually occurs in women in their mid-sixties.
Other lesions
Other lesions, such as adenocarcinoma (of the Bartholin glands, for example) or sarcoma, may cause vulvar cancer as well.[13] Erythroplasia or Queyrat, typically found on the penis may affect the vulvae in females.[14]
Risk factors
Although the exact cause of vulvar cancer isn't known, certain factors appear to increase your risk of the disease.
- Increasing age
- Exposure to human papillomavirus
- Smoking
- Being infected with the human immunodeficiency virus (HIV)
- Having a history of precancerous conditions of the vulva
- Having a skin condition involving the vulva
Signs and symptoms
Many malignancies can develop in vulvar structures.[15] The signs and symptoms can include:
- Itching, burn, or bleeding on the vulva that does not go away.
- Changes in the color of the skin of the vulva, so that it looks redder or whiter than is normal.
- Skin changes in the vulva, including what looks like a rash or warts.
- Sores, lumps, or ulcers on the vulva that do not go away.
- Pain in the pelvis, especially during urination or sex.[16]
Typically, a lesion presents in the form of a lump or ulcer on the labia majora and may be associated with itching, irritation, local bleeding or discharge, in addition to pain with urination or pain during sexual intercourse. The labia minora, clitoris, perineum and mons are less commonly involved. Due to modesty or embarrassment, patients may put off seeing a doctor.[17]
Melanomas tend to display the typical asymmetry, uneven borders and dark discoloration as do melanomas in other parts of the body.
Adenocarcinoma can arise from the Bartholin gland and present with a painful lump.[18]
Causes
Some conditions such as lichen sclerosus, squamous dysplasia or chronic vulvar itching may precede cancer. In younger women affected with vulvar cancer, risk factors include low socioeconomic status, multiple sexual partners, cigarette use and cervical cancer.[9] Patients that are infected with HIV tend to be more susceptible to vulvar cancer as well. Human papillomavirus (HPV) infection is associated with vulvar cancer.[19]
Diagnosis
Examination of the vulva is part of the gynecologic evaluation and should include a thorough inspection of the perineum, including areas around the clitoris and urethra, and palpation of the Bartholin's glands.[20] The exam may reveal an ulceration, lump or mass in the vulvar region. Any suspicious lesions need to be sampled, or biopsied. This can generally be done in an office setting under local anesthesia. Small lesions can be removed under local anesthesia as well. Additional evaluation may include a chest X-ray, an intravenous pyelogram, cystoscopy or proctoscopy, as well as blood counts and metabolic assessment.
Differential diagnosis
Other cancerous lesions in the differential diagnosis include Paget's disease of the vulva and vulvar intraepithelial neoplasia (VIN). Non-cancerous vulvar diseases include lichen sclerosus, squamous cell hyperplasia, and vulvar vestibulitis. A number of diseases cause infectious lesions including herpes genitalis, human papillomavirus, syphilis, chancroid, granuloma inguinale, and lymphogranuloma venereum.
Staging
Anatomical staging supplemented preclinical staging starting in 1988. FIGO’s revised TNM classification system uses tumor size (T), lymph node involvement (N) and presence or absence of metastasis (M) as criteria for staging. Stages I and II describe the early stages of vulvar cancer that still appear to be confined to the site of origin. Stage III cancers include greater disease extension to neighboring tissues and inguinal lymph nodes on one side. Stage IV indicates metastatic disease to inguinal nodes on both sides or distant metastases.[21]
- Illustrations showing stages of vulvar cancer'"`UNIQ--ref-00000000-QINU`"'
 Stage 1A and 1B vulvar cancer
Stage 1A and 1B vulvar cancer Stage 2 vulvar cancer
Stage 2 vulvar cancer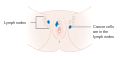 Stage 3 vulvar cancer
Stage 3 vulvar cancer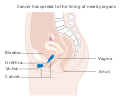 Stage 4A vulvar cancer
Stage 4A vulvar cancer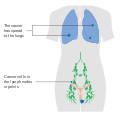 Stage 4B vulvar cancer
Stage 4B vulvar cancer
Treatment
Staging and treatment are generally handled by an oncologist familiar with gynecologic cancer. Surgery is a mainstay of therapy depending on anatomical staging and is usually reserved for cancers that have not spread beyond the vulva.[21] Surgery may involve a wide local excision, radical partial vulvectomy, or radical complete vulvectomy with removal of vulvar tissue, inguinal and femoral lymph nodes. In cases of early vulvar cancer, the surgery may be less extensive and consist of wide excision or a simple vulvectomy. Surgery is significantly more extensive when the cancer has spread to nearby organs such as the urethra, vagina, or rectum. Complications of surgery include wound infection, sexual dysfunction, edema and thrombosis, as well as lymphedema secondary to dissected lymph nodes.[22]
Sentinel lymph node (SLN) dissection is the identification of the main lymph node(s) draining the tumor, with the aim of removing as few nodes as possible, decreasing the risk of adverse effects. Location of the sentinel node(s) may require the use of technetium(99m)-labeled nano-colloid, or a combination of technetium and 1% isosulfan blue dye, wherein the combination may reduce the number of women with "'missed"' groin node metastases compared with technetium only.[22]

Radiation therapy may be used in more advanced vulvar cancer cases when disease has spread to the lymph nodes and/or pelvis. It may be performed before or after surgery. Chemotherapy is not usually used as primary treatment but may be used in advanced cases with spread to the bones, liver or lungs. It may also be given at a lower dose together with radiation therapy.[23]
Women with vulvar cancer should have routine follow-up and exams with their oncologist, often every 3 months for the first 2–3 years after treatment. They should not have routine surveillance imaging to monitor the cancer unless new symptoms appear or tumor markers begin rising.[24] Imaging without these indications is discouraged because it is unlikely to detect a recurrence or improve survival and is associated with its own side effects and financial costs.[24]
Prognosis
Overall, five-year survival rates for vulvar cancer are around 78%[9] but may be affected by individual factors including cancer stage, cancer type, patient age and general medical health. Five-year survival is greater than 90% for patients with stage I lesions but decreases to 20% when pelvic lymph nodes are involved. Lymph node involvement is the most important predictor of prognosis.[25] Thus, early diagnosis is important.
Epidemiology
Vulvar cancer causes less than 1% of all cancer cases and deaths but around 6% of all gynecologic cancers diagnosed in the UK. Around 1,200 women were diagnosed with the disease in 2011, and 400 women died in 2012.[26] Vulvar cancer causes about 0. 6% of all cancer cases[27] but 5% of gynecologic cancers in the United States.[28] About 4900 cases are diagnosed each year in the United States.[29]
References
- ↑ "American Cancer Society: What are the key statistics about vulvar cancer?". www. cancer.org. Retrieved 6 November 2014.
- ↑ "Vulvar Cancer Treatment". National Cancer Institute. Retrieved 2015-04-14.
- ↑ "Vulvar Cancer Treatment". National Cancer Institute. Retrieved 2015-04-14.
- ↑ "What is vulvar cancer?". cancer.org. Retrieved 2015-04-14.
- ↑ "What is Vulvar Cancer?". Society of Gynecologic Oncology. Retrieved 19 November 2014.
- ↑ "American Cancer Society" (PDF). Retrieved 30 April 2014.
- ↑ "SEER Stat Fact Sheets: Vulvar Cancer". NCI. Retrieved 18 June 2014.
- ↑ "Vulvar Cancer—October 1, 2002—American Family Physician". Retrieved 2010-03-06.
- 1 2 3 4 5 6 Hoffman, Barbara; Schorge, John; Schaffer, Joseph; Halvorson, Lisa; Bradshaw, Karen; Cunningham, Gary (2012). Williams Gynecology (2nd ed.). The McGraw-Hill Company, Inc. ISBN 978-0-07-171672-7.
- ↑ "American Cancer Society: What is Vulvar Cancer?". www.cancer.org. Retrieved 2014-06-11.
- ↑ Evans, RA (1994). "Review and current perspectives of cutaneous malignant melanoma.". Journal of the American College of Surgeons. 179: 764–7. PMID 7952494.
- ↑ DeCherney, Alan H.; Nathan, Lauren; Laufer, Neri; Roman, Ashley S. (2013). Current Diagnosis and Treatment: Obstetrics and Gynecology (11th ed.). USA: The McGraw-Hill Companies, Inc. ISBN 978-0-07-163856-2.
- ↑ Visco, AG; Del Priore, G (1996). "Postmenopausal bartholin gland enlargement: a hospital-based cancer risk assessment.". Obstet Gynecol. 87.
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. p. 1050. ISBN 1-4160-2999-0.
- ↑ Hoffman, Barbara (2012). Williams Gynecology (2nd. ed.). New York: McGraw-Hill Medical. pp. 794–806. ISBN 9780071716727.
- ↑ "What Are the Symptoms of Vaginal and Vulvar Cancers?". CDC. 13 March 2014. Retrieved 2016-03-26.
- ↑ Zacur, H; Genadry, R; Woodruff, JD (1980). "The patient-at-risk for development of vulvar cancer". Gynecol Oncol. 9: 199–208. doi:10.1016/0090-8258(80)90028-1. PMID 7372192.
- ↑ Copeland, LJ; Sneige, N; Gershenson, DM; McGuffee, VB; Abdul-Karim, F; Rutledge, FN (1986). "Bartholin gland carcinoma". Obstet Gynecol. 67: 794–801. doi:10.1097/00006250-198606000-00009. PMID 3010205.
- ↑ Zweizig, Susan; Korets, Sharmilee; Cain, Joanna M. (2014). "Key concepts in management of vulvar cancer". Best Practice & Research Clinical Obstetrics & Gynaecology. 28 (7): 959–966. doi:10.1016/j.bpobgyn.2014.07.001. ISSN 1521-6934.
- ↑ "Vulvar Cancer". Gynecologic Neoplasms. Armenian Health Network, Health.am. 2005. Retrieved 2007-11-08.
- 1 2 International Federation of Gynecologists and Obstetricians (FIGO) (2000). "Staging classification and clinical practice guidelines of gynaecologic cancers" (PDF). Archived from the original (PDF) on 2006-04-23. Retrieved 2006-10-13.
- 1 2 Lawrie, Theresa A; Patel, Amit; Martin-Hirsch, Pierre PL; Bryant, Andrew; Ratnavelu, Nithya DG; Naik, Raj; Ralte, Angela; Patel, Amit (2014). "Sentinel node assessment for diagnosis of groin lymph node involvement in vulval cancer". Protocols. doi:10.1002/14651858.CD010409.pub2.
- ↑ "What are the treatment options?". Society of Gynecologic Oncology. Retrieved 19 November 2014.
- 1 2 Society of Gynecologic Oncology (February 2014), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, Society of Gynecologic Oncology, retrieved 19 February 2013
- ↑ Farias-Eisner, R; Cirisano, FD; Grouse, D (1994). "Conservative and individualized surgery for early squamous carcinoma of the vulva: the treatment of choice for stage I and II (T1–2N0–1M0) disease". Gynecologic Oncology. 53: 55–58. doi:10.1006/gyno.1994.1087. PMID 8175023.
- ↑ "Vulval cancer statistics". Cancer Research UK. Retrieved 28 October 2014.
- ↑ "American Cancer Society: What are the key statistics about vulvar cancer?". www.cancer.org. Retrieved 12 May 2015.
- ↑ "Vulvar Cancer Treatment". National Cancer Institute. Retrieved 12 May 2015.
- ↑ Siegel, R; Ma, J; Zou, Z; Jemal, A (2014). "Cancer statistics, 2014.". CA Cancer J Clin. 64: 9–29. doi:10.3322/caac.21208. PMID 24399786.
External links
- Guide by the American Cancer Society
- Information from the National Cancer Institute
- Vulvar Cancer. Timothy P. Canavan and Donna Cohen. Am Fam Physician 2002;66:1269–74,1276. Review article for general practitioners.
- Cancer.Net: Vulvar Cancer
- Oncolex Cancer Encyclopedia: Vulvar Cancer