Spondylolisthesis
| Spondylolisthesis | |
|---|---|
 | |
| X-ray of the lateral lumbar spine with a grade III spondylolisthesis at the L5-S1 level. | |
| Classification and external resources | |
| Specialty | Orthopedics |
| ICD-10 | M43.1, Q76.2 |
| ICD-9-CM | 738.4, 756.12 |
| OMIM | 184200 |
| DiseasesDB | 12318 |
| MedlinePlus | 001260 |
| eMedicine | radio/651 |
| Patient UK | Spondylolisthesis |
| MeSH | D013168 |
Spondylolisthesis /ˌspɒndɪloʊlɪsˈθisɪs/ SPON-dill-oh-lis-THEE-sis is the forward displacement of a vertebral bone in relation to the natural curve of the spine, most commonly occurring after a fracture, and most often the fifth lumbar vertebra.[1] Backward displacement is referred to as retrolisthesis. When occurring in conjunction with scoliosis, the shortened term "olisthesis," may sometimes be used instead. [2]
A hangman's fracture is a specific type of spondylolisthesis where the second cervical vertebra (C2) is displaced anteriorly relative to the C3 vertebra due to fractures of the C2 vertebra's pedicles.
Signs and symptoms
Symptoms of spondylolisthesis include:
- A general stiffening of the back and a tightening of the hamstrings, with a resulting change in both posture and gait.
- A leaning-forward or semi-kyphotic posture may be seen, due to compensatory changes.
- A "waddle" may be seen in more advanced causes, due to compensatory pelvic rotation due to decreased lumbar spine rotation.
- A result of the change in gait is often a noticeable atrophy in the gluteal muscles due to lack of use.
- Generalized lower-back pain may also be seen, with intermittent shooting pain from the buttocks to the posterior thigh, and/or lower leg via the sciatic nerve.
Other symptoms may include tingling and numbness. Coughing and sneezing can intensify the pain. An individual may also note a "slipping sensation" when moving into an upright position. Sitting and trying to stand up may be painful and difficult.[3][4]
Classification
Spondylolisthesis is categorized into five types:[5]
- Isthmic spondylolisthesis is the most common form; also called spondylolytic spondylolisthesis, it occurs with a reported prevalence of 5–7 percent in the US population. A slip or fracture of the intravertebral joint is usually acquired between the ages of 6 and 16 years, but remains unnoticed until adulthood. Roughly 90 percent of these isthmic slips are low-grade (less than 50 percent slip) and 10 percent are high-grade (greater than 50 percent slip).[5] It is divided into three subtypes:[6]
- A: pars fatigue fracture
- B: pars elongation due to multiple healed stress fx
- C: pars acute fracture
- Degenerative spondylolisthesis is a disease of the older adult that develops as a result of facet arthritis and joint remodeling. Joint arthritis, and ligamentum flavum weakness, may result in slippage of a vertebra. Degenerative forms are more likely to occur in women, persons older than fifty, and African Americans.[5]
- Traumatic spondylolisthesis is rare and results from acute fractures in the neural arch, other than the pars.[7]
- Pathologic spondylolisthesis has been associated with damage to the posterior elements from metastases or metabolic bone disease. These slips have been reported in cases of Paget's disease of bone, tuberculosis, giant-cell tumors, and tumor metastases.[8]
- Dysplastic results from congenital abnormalities of the upper sacral facets or inferior facets of the fifth lumbar vertebra, and accounts for 14% to 21% of all spondylolisthesis.[9]
 X-ray picture of a grade 1 isthmic spondylolisthesis at L4-5
X-ray picture of a grade 1 isthmic spondylolisthesis at L4-5 MRI of L5-S1 spondylolisthesis
MRI of L5-S1 spondylolisthesis X-ray of a grade 4 spondylolisthesis at L5-S1 with spinal misalignment indicated
X-ray of a grade 4 spondylolisthesis at L5-S1 with spinal misalignment indicated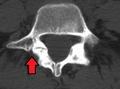 Spondylolisthesis L5/S1
Spondylolisthesis L5/S1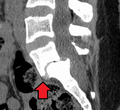 Spondylolisthesis L5/S1
Spondylolisthesis L5/S1 Spondylolisthesis L5/S1. Blue arrow normal pars interarticularis. Red arrow is a break in pars interarticularis
Spondylolisthesis L5/S1. Blue arrow normal pars interarticularis. Red arrow is a break in pars interarticularis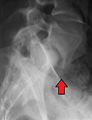 Spondylolisthesis L5/S1
Spondylolisthesis L5/S1
Treatment
Conservative management
Patients with symptomatic isthmic spondylolisthesis are initially offered conservative treatment consisting of activity modification, pharmacological intervention, and a physical therapy consultation.
- Physical therapy can evaluate and address postural and compensatory movement abnormalities.
- Anti-inflammatory medications (NSAIDS) in combination with paracetamol (Tylenol) can be tried initially. If a severe radicular component is present, a short course of oral steroids such as Prednisone or Methylprednisolone can be considered. Epidural steroid injections, either interlaminal or transforaminal, performed under fluoroscopic guidance can help with severe radicular (leg) pain. Lumbosacral orthoses may be of benefit for some patients but should be used on a temporary basis to prevent spinal muscle atrophy and loss of proprioception.
Surgical
Degenerative spondylolisthesis with spinal stenosis is one of the most common indications for spine surgery (typically a laminectomy) among older adults.[10]
History
Spondylolisthesis was first described in 1782 by Belgian obstetrician Herbinaux.[11] He reported a bony prominence anterior to the sacrum that obstructed the vagina of a small number of patients.[12] The term “spondylolisthesis” was coined in 1854 from the Greek σπονδυλος, "spondylos" = "vertebra" and ὀλισθός "olisthos" = "slipperiness," "a slip."[13]
See also
References
- ↑ Foreman P, Griessenauer CJ, Watanabe K, Conklin M, Shoja MM, Rozzelle CJ, Loukas M, Tubbs RS (2013). "L5 spondylolysis/spondylolisthesis: a comprehensive review with an anatomic focus". Child's Nervous System. 29 (2): 209–16. doi:10.1007/s00381-012-1942-2. PMID 23089935.
- ↑ "Natural History of Adult Scoliosis".
- ↑ http://orthoinfo.aaos.org/topic.cfm?topic=A00588[]
- ↑ http://www.webmd.com/back-pain/tc/spondylolisthesis-topic-overview[]
- 1 2 3 "Adult Spondylolisthesis in the Low Back". American Academy of Orthopaedic Surgeons. Retrieved 9 June 2013.
- ↑ http://www.orthobullets.com/spine/2038/adult-isthmic-spondylolisthesis[]
- ↑ Syrmou E, Tsitsopoulos PP, Marinopoulos D, Tsonidis C, Anagnostopoulos I, Tsitsopoulos PD (2010). "Spondylolysis: a review and reappraisal". Hippokratia. 14 (1): 17–21. PMC 2843565
 . PMID 20411054.
. PMID 20411054. - ↑ http://www.basicspine.com/blog/spondylolisthesis-displacement-lower-spine-injury-age/[]
- ↑ Leone LD, Lamont DW (1999). "Diagnosis and treatment of severe dysplastic spondylolisthesis". The Journal of the American Osteopathic Association. 99 (6): 326–8. doi:10.7556/jaoa.1999.99.6.326. PMID 10405520.
- ↑ Grabias S (1980). "Current concepts review. The treatment of spinal stenosis". The Journal of Bone and Joint Surgery. American Volume. 62 (2): 308–13. PMID 6987238.
- ↑ Newman PH (1955). "Spondylolisthesis, its cause and effect". Annals of the Royal College of Surgeons of England. 16 (5): 305–23. PMC 2377893. PMID 14377314.
- ↑ Garrigues, Henry Jacques (1902). "Spondylolisthesic pelvis". A textbook of the science and art of obstetrics. pp. 490–93. OCLC 654149619.
- ↑ "Isthmic Spondylolisthesis and Spondylolysis".