Campylobacter jejuni
| Campylobacter jejuni | |
|---|---|
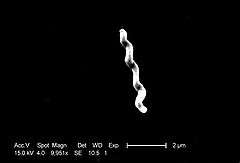 | |
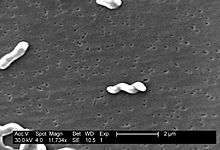
| Scanning electron micrograph of C. jejuni demonstrating the characteristic curve rod shape of the organism | |
| Scientific classification | |
| Domain: | Bacteria |
| Phylum: | Proteobacteria |
| Class: | Epsilonproteobacteria |
| Order: | Campylobacterales |
| Family: | Campylobacteraceae |
| Genus: | Campylobacter |
| Species: | C. jejuni |
| Binomial name | |
| Campylobacter jejuni (Jones et al., 1931) Veron & Chatelain, 1973 | |
Campylobacter jejuni (CAM-puh-low-back-ter juh-JUNE-eye) is one of the most common causes of food poisoning in the United States. The vast majority of cases occur as isolated events, not as part of recognized outbreaks.[1] Active surveillance through the Foodborne Diseases Active Surveillance Network (FoodNet) indicates that about 14 cases are diagnosed each year for each 100,000 persons in the population.[2] Campylobacter jejuni is in a genus of bacteria that is among the most common causes of bacterial infections in humans worldwide. The name means "curved rod", deriving from the Greek campylos (curved) and baktron (rod). It has been noted that there "is wide diversity in the genus. The species are metabolically and genetically different to the extent that one can question whether one genus is adequate to house all of the species." Of its many species, C. jejuni is considered one of the most important from both a microbiological and public health perspective.[3]
C. jejuni is also commonly found in animal feces. Campylobacter is a helical-shaped, nonspore-forming, Gram-negative, microaerophilic, nonfermenting bacterium forming motile rods with a single polar flagellum, which are also oxidase-positive and grow optimally at 37 to 42 °C.[4][5][6][7] This species of pathogenic bacteria is one of the most common causes of human gastroenteritis in the world. Food poisoning caused by Campylobacter species can be severely debilitating, but is rarely life-threatening. It has been linked with subsequent development of Guillain–Barré syndrome, which usually develops two to three weeks after the initial illness.[8]
Disease
Campylobacteriosis is an infectious disease caused by bacteria of the genus Campylobacter. In most people who become ill with campylobacteriosis, symptoms develop within two to five days of exposure to the organism and illness typically lasts seven days following onset.[2] Infection with C. jejuni usually results in enteritis, which is characterised by abdominal pain, diarrhea, fever, and malaise. Diarrhea itself can vary in severity from loose to bloody stools. The disease is usually self-limiting. However, it does respond to antibiotics. Severe (accompanying fevers, blood in stools) or prolonged cases may require erythromycin, azithromycin, ciprofloxacin, or norfloxacin. Fluid replacement may be required for serious cases.[2]
Pathogenesis
Studies on the pathogenesis of C. jejuni show that for this organism to cause disease, the susceptibility of the host and the relative virulence of the infecting strain are both important. Infection results from the ingestion of contaminated food or water, and the infective dose can be as low as 800 organisms. To initiate infection, the organism must penetrate the gastrointestinal mucus, which it does using its high motility and spiral shape. The bacteria must then adhere to the gut enterocytes and can then induce diarrhea by toxin release. C. jejuni releases several different toxins, mainly enterotoxin and cytotoxins, which vary from strain to strain and correlate with the severity of the enteritis. During infection, levels of all immunoglobulin classes rise. Of these, IgA is the most important because it can cross the gut wall. IgA immobilises organisms, causing them to aggregate and activate complement, and also gives short-term immunity against the infecting strain of organism.[9] The bacteria colonize the small and large intestines, causing inflammatory diarrhea with fever. Stools contain leukocytes and blood. The role of toxins in pathogenesis is unclear. C jejuni antigens that cross-react with one or more neural structures may be responsible for triggering the Guillain–Barré syndrome.[7]
Sources
C. jejuni is commonly associated with poultry, and it naturally colonises the digestive tract of many bird species. One study found that 30% of European starlings in farm settings in Oxfordshire, United Kingdom, were carriers of C. jejuni. It is also common in cattle, and although it is normally a harmless commensal of the gastrointestinal tract in these animals, it can cause campylobacteriosis in calves. It has also been isolated from wombat and kangaroo feces, being a cause of bushwalkers' diarrhea. Contaminated drinking water and unpasteurized milk provide an efficient means for distribution. Contaminated food is a major source of isolated infections, with incorrectly prepared meat and poultry as the primary source of the bacteria.[10] Moreover, surveys show that 20 to 100% of retail chickens are contaminated. This is not overly surprising, since many healthy chickens carry these bacteria in their intestinal tracts. Raw milk is also a source of infections. The bacteria are often carried by healthy cattle and by flies on farms. Unchlorinated water may also be a source of infections. However, properly cooking chicken, pasteurizing milk, and chlorinating drinking water kill the bacteria.[11]
Possible complications
Local complications of Campylobacter infections occur as a result of direct spread from the gastrointestinal tract and can include cholecystitis, pancreatitis, peritonitis, and massive gastrointestinal hemorrhage. Extraintestinal manifestations of Campylobacter infection are quite rare and may include meningitis, endocarditis, septic arthritis, osteomyelitis, and neonatal sepsis. Bacteremia is detected in <1% of patients with Campylobacter enteritis and is most likely to occur in patients who are immunocompromised or among the very young or very old.[12] Transient bacteremia in immunocompetent hosts with C. jejuni enteritis may be more common, but not detected because most strains are rapidly cleared by the killing action of normal human serum and because blood cultures are not routinely performed for patients with acute gastrointestinal illness. Serious systemic illness caused by Campylobacter infection rarely occurs, but can lead to sepsis and death. The case-fatality rate for Campylobacterinfection is 0.05 per 1000 infections. For instance, one major possible complication that C. jejuni can cause is Guillain–Barré syndrome, which a sizeable percentage of persons who suffer this can cause a person a neuromuscular paralysis. Over time, the paralysis is to some extent typically reversible; nonetheless, about 20% of patients with GBS are left disabled, and around 5% die. Another chronic condition that may be associated with Campylobacter infection is formerly known as Reiter's syndrome, a form of reactive arthritis.[13] Reactive arthritis is a complication strongly associated with a particular genetic make-up, that is, persons who have the human lymphocyte antigen B27 (HLA-B27) are most susceptible. Most often, the symptoms of reactive arthritis can occur up to several weeks after infections.[3][14]
Epidemiology
Frequency
United States
An estimated 2 million cases of Campylobacter enteritis occur annually, accounting for 5–7% of cases of gastroenteritis.[15] Campylobacter organisms have a large animal reservoir, with up to 100% of poultry, including chickens, turkeys, and waterfowl, having asymptomatic intestinal infections. The major reservoirs of C. fetus are cattle and sheep. Nonetheless, the incidence of Campylobacter infections has been declining. Changes in the incidence of culture-confirmed Campylobacter infections have been monitored by the Foodborne Diseases Active Surveillance Network (FoodNet) since 1996. In 2010, Campylobacter incidence showed a 27% decrease compared with 1996–1998. In 2010, the incidence was 13.6 cases per 100,000 population, and this did not change significantly compared with 2006–2008.[1][16]
International
C. jejuni infections are extremely common worldwide, although exact figures are not available. New Zealand reported the highest national campylobacteriosis rate, which peaked in May 2006 at 400 per 100,000 population.[2][16]
Sex
Campylobacter organisms are isolated more frequently from males than females. Homosexual men appear to be at increased risk for infection with atypical Campylobacter species such as Helicobacter cinaedi and Helicobacter fennelliae.[16]
Age
Campylobacter infections can occur in all age groups. Studies show a peak incidence in children younger than 1 year and in persons aged 15–29 years. The age-specific attack rate is highest in young children. In the United States, the highest incidence of Campylobacter infection in 2010 was in children younger than 5 years and was 24.4 cases per 100,000 population,[1] However, the rate of fecal cultures positive for Campylobacter species is greatest in adults and older children.[16]
Treatment
Patients with Campylobacter infection should drink plenty of fluids as long as the diarrhea lasts to maintain hydration. One must drink plenty of fluids and get rest. If he or she cannot drink enough fluids to prevent dehydration or if the symptoms are severe, medical help is indicated. In more severe cases, certain antibiotics can be used and can shorten the duration of symptoms if given early in the illness.[1] Moreover, maintenance of electrolyte balance, not antibiotic treatment, is the cornerstone of treatment for Campylobacter enteritis. Indeed, most patients with this infection have a self-limited illness and do not require antibiotics at all. Nevertheless, antibiotics should be used in specific clinical circumstances. These include high fevers, bloody stools, prolonged illness (symptoms that last >1 week), pregnancy, infection with HIV, and other immunocompromised states.[14]
Prevention
Some simple food-handling practices can help prevent Campylobacter infections.[2]
- Cook all poultry products thoroughly. Make sure that the meat is cooked throughout (no longer pink) and any juices run clear. All poultry should be cooked to reach a minimum internal temperature of 165 °F (74 °C).
- If served undercooked poultry in a restaurant, send it back for further cooking.
- Wash hands with soap before preparing food.
- Wash hands with soap after handling raw foods of animal origin and before touching anything else.
- Prevent cross-contamination in the kitchen by using separate cutting boards for foods of animal origin and other foods and by thoroughly cleaning all cutting boards, countertops, and utensils with soap and hot water after preparing raw food of animal origin.
- Do not drink unpasteurized milk or untreated surface water.
- Make sure that persons with diarrhea, especially children, wash their hands carefully and frequently with soap to reduce the risk of spreading the infection.
- Wash hands with soap after contact with pet feces.
Genome
The genome of C. jejuni strain NCTC11168 was published in 2000, revealing 1,641,481 base pairs (30.6% G+C) predicted to encode 1,654 proteins and 54 stable RNA species. The genome is unusual in that virtually no insertion sequences or phage-associated sequences and very few repeat sequences are found. One of the most striking findings in the genome was the presence of hypervariable sequences. These short homopolymeric runs of nucleotides were commonly found in genes encoding the biosynthesis or modification of surface structures, or in closely linked genes of unknown function. The apparently high rate of variation of these homopolymeric tracts may be important in the survival strategy of C. jejuni.[17]
Initial transposon mutagenesis screens revealed 195 essential genes, although this number is likely to go up with additional analysis.[18]
Natural genetic transformation
C. jejuni is naturally competent for genetic transformation.[19] Natural genetic transformation is a sexual process involving DNA transfer from one bacterium to another through the intervening medium, and the integration of the donor sequence into the recipient genome by homologous recombination. C. jejuni freely takes up foreign DNA harboring genetic information responsible for antibiotic resistance.[19] Antibiotic resistance genes are more frequently transferred in biofilms than between planktonic cells (single cells that float in liquid media).
Laboratory characteristics
| Characteristic | Result |
|---|---|
| Growth at 25 °C | − |
| Growth at 35–37 °C | + |
| Growth at 42 °C | + |
| Nitrate reduction | + |
| Catalase test | + |
| Oxidase test | + |
| Growth on MacConkey agar | + |
| Motility (wet mount) | + |
| Glucose utilization | − |
| Hippurate hydrolysis | + |
| Resistance to nalidixic acid | − |
| Resistance to cephalothin | + |
Under light microscopy, C. jejuni has a characteristic "sea-gull" shape as a consequence of its helical form. Campylobacter is grown on specially selective "CAMP" agar plates at 42 °C, the normal avian body temperature, rather than at 37 °C, the temperature at which most other pathogenic bacteria are grown. Since the colonies are oxidase positive, they usually only grow in scanty amounts on the plates. Microaerophilic conditions are required for luxurious growth. A selective blood agar medium (Skirrow's medium) can be used. Greater selectivity can be gained with an infusion of a cocktail of antibiotics: vancomycin, polymixin-B, trimethoprim, and actidione ([Preston's agar]),[20] and growth under microaerophilic conditions at 42 °C.
References
- 1 2 3 4 Foodsafety.gov. "Campylobacter". www.foodsafety.gov. Retrieved 2016-04-18.
- 1 2 3 4 5 "Food Safety: Campylobacter". U.S. Centers for Disease Control and Prevention. Retrieved 2016-04-18.
- 1 2 "Campylobacter jejuni | Campylobacter Food Poisoning". www.about-campylobacter.com. Retrieved 2016-04-18.
- ↑ Ryan KJ, Ray CG, eds. (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. ISBN 0-8385-8529-9.
- ↑ Online Bacteriological Analytical Manual, Chapter 7: Campylobacter
- ↑ Gorbach, Sherwood L.; Falagas, Matthew, eds. (2001). The 5 minute infectious diseases consult (1st ed.). Lippincott Williams & Wilkins. ISBN 0-683-30736-3."Multiple Campylobacter Genomes Sequenced". 2005-01-04. Retrieved 2007-07-27.
- 1 2 Perez-Perez, Guillermo I.; Blaser, Martin J. (1996-01-01). Baron, Samuel, ed. Campylobacter and Helicobacter (4th ed.). Galveston (TX): University of Texas Medical Branch at Galveston. ISBN 0963117211. PMID 21413331.
- ↑ Fujimoto S, Amako K. Guillain–Barré syndrome and Campylobacter jejuni infection. Lancet 1990;35:1350.
- ↑ Wallis, M. R. (1994-03-01). "The pathogenesis of Campylobacter jejuni". British Journal of Biomedical Science. 51 (1): 57–64. ISSN 0967-4845. PMID 7841837.
- ↑ F M Colles, N D McCarthy, J C Howe, C L Devereux, A G Gosler, and M C J Maiden Dynamics of Campylobacter colonization of a natural host, Sturnus vulgaris (European Starling) Environ Microbiol. 2009 January; 11(1): 258–267. doi:10.1111/j.1462-2920.2008.01773.x.
- ↑ Nutrition, Center for Food Safety and Applied. "Bad Bug Book - BBB - Campylobacter jejuni". www.fda.gov. Retrieved 2016-04-18.
- ↑ Skirrow MB, Jones DM, Sutcliffe E, Benjamin J. Campylobacter bacteraemia in England and Wales, 1981–1991. Epidemiol Infect 1993;110:567–73.
- ↑ "What is Reactive Arthritis?". Reactive Arthritis.
- 1 2 Acheson, David; Allos, Ban Mishu (2001-04-15). "Campylobacter jejuni Infections: Update on Emerging Issues and Trends". Clinical Infectious Diseases. 32 (8): 1201–1206. doi:10.1086/319760. ISSN 1058-4838. PMID 11283810.
- ↑ Jennifer Lynn Bonheur. BS Anand, ed. "Bacterial Gastroenteritis". Medscape Reference.
- 1 2 3 4 "Campylobacter Infections: Background, Pathophysiology, Epidemiology".
- ↑ Parkhill, J.; Wren, B. W.; Mungall, K.; Ketley, J. M.; Churcher, C.; Basham, D.; Chillingworth, T.; Davies, R. M.; Feltwell, T.; Holroyd, S.; Jagels, K.; Karlyshev, A. V.; Moule, S.; Pallen, M. J.; Penn, C. W.; Quail, M. A.; Rajandream, M. A.; Rutherford, K. M.; Van Vliet, A. H. M.; Whitehead, S.; Barrell, B. G. (2000). "The genome sequence of the food-borne pathogen Campylobacter jejuni reveals hypervariable sequences". Nature. 403 (6770): 665–8. doi:10.1038/35001088. PMID 10688204.
- ↑ Stahl, M; Stintzi, A (2011). "Identification of essential genes in C. Jejuni genome highlights hyper-variable plasticity regions". Functional & Integrative Genomics. 11 (2): 241–57. doi:10.1007/s10142-011-0214-7. PMID 21344305.
- 1 2 Bae J, Oh E, Jeon B (2014). "Enhanced transmission of antibiotic resistance in Campylobacter jejuni biofilms by natural transformation". Antimicrob. Agents Chemother. 58 (12): 7573–5. doi:10.1128/AAC.04066-14. PMC 4249540
 . PMID 25267685.
. PMID 25267685. - ↑ FJ Bolton; L Robertson (1982). "A selective medium for isolating Campylobacter jejuni/coli" (pdf). J Clin Pathol. 35: 462–476. doi:10.1136/jcp.35.4.462.
External links
- Campylobacter jejuni genomes and related information at PATRIC, a Bioinformatics Resource Center funded by NIAID
- Current research on Campylobacter jejuni at the Norwich Research Park
- Type strain of Campylobacter jejuni at BacDive - the Bacterial Diversity Metadatabase