Tetralogy of Fallot
| Tetralogy of Fallot | |
|---|---|
| Synonyms | Fallot’s syndrome, Fallot’s tetrad, Steno-Fallot tetralogy[1] |
 | |
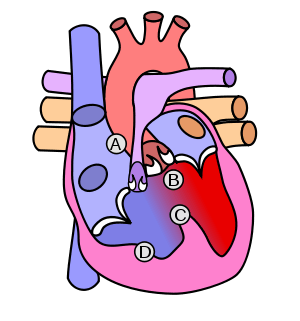
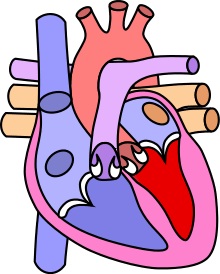
| Diagram of a healthy heart and one with tetralogy of Fallot | |
| Classification and external resources | |
| Specialty | Cardiac surgery, pediatrics |
| ICD-10 | Q21.3 |
| ICD-9-CM | 745.2 |
| OMIM | 187500 |
| DiseasesDB | 4660 |
| MedlinePlus | 001567 |
| eMedicine | emerg/575 |
| Patient UK | Tetralogy of Fallot |
| MeSH | D013771 |
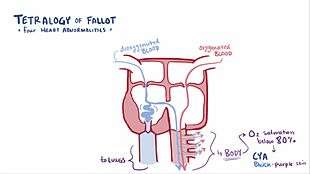
Tetralogy of Fallot (TOF) is a congenital heart defect that is present at birth.[2] Symptoms include episodes of bluish color to the skin. When affected babies cry or have a bowel movement, they may develop a "tet spell" where they turn very blue, have difficulty breathing, become limp, and occasionally lose consciousness. Other symptoms may include a heart murmur, finger clubbing, and easy tiring upon breastfeeding.[3]
The cause is typically not known. Risk factors include a mother who uses alcohol, has diabetes, is over the age of 40, or gets rubella during pregnancy. It may also be associated with Down syndrome.[4] Classically there are four defects:[2]
- a ventricular septal defect, a hole between the two ventricles
- pulmonary stenosis, narrowing of the exit from the right ventricle
- right ventricular hypertrophy, enlargement of the right ventricle
- an overriding aorta, which allows blood from both ventricles to enter the aorta
TOF is typically treated by open heart surgery in the first year of life. Timing of surgery depends on the baby's symptoms and size. The procedure involves increasing the size of the pulmonary valve and pulmonary arteries and repairing the ventricular septal defect. In babies who are too small a temporary surgery may be done with plans for a second surgery when the baby is bigger.[5] Most people who are affected live to be adults.[2] Long-term problems may include an irregular heart rate and pulmonary regurgitation.[6]
TOF occurs in about 1 in 2,000 newborns.[2] Males and females are affected equally.[2] It is the most common complex congenital heart defect.[7] It was initially described in 1671 by Niels Stensen. A further description occurred in 1888 by the French physician Étienne-Louis Arthur Fallot, after whom it is named.[1] The first surgical repair was carried out in 1954.[6]
Signs and symptoms

Tetralogy of Fallot results in low oxygenation of blood due to the mixing of oxygenated and deoxygenated blood in the left ventricle via the ventricular septal defect (VSD) and preferential flow of the mixed blood from both ventricles through the aorta because of the obstruction to flow through the pulmonary valve. This is known as a right-to-left shunt. The primary symptom is low blood oxygen saturation with or without cyanosis from birth or developing in the first year of life. If the baby is not cyanotic then it is sometimes referred to as a "pink tet".[8] Other symptoms include a heart murmur which may range from almost imperceptible to very loud, difficulty in feeding, failure to gain weight, retarded growth and physical development, dyspnea on exertion, clubbing of the fingers and toes, and polycythemia.
Tet spells
Children with tetralogy of Fallot may develop "tet spells". These are acute hypoxia spells, characterized by shortness of breath, cyanosis, agitation, and loss of consciousness. This may be initiated by any event leading to decreased oxygen saturation or that causes decreased systemic vascular resistance, leading to increased venous return, which in turn leads to increased shunting through the ventricular septal defect.
Tet spells are characterized by a sudden, marked increase in cyanosis followed by syncope, and may result in hypoxic brain injury and death.
Older children will often squat during a tet spell. This increases systemic vascular resistance and allows for a temporary reversal of the shunt. It increases pressure on the left side of the heart, decreasing the right to left shunt thus decreasing the amount of deoxygenated blood entering the systemic circulation.[9][10]
Cause
Its cause is thought to be due to environmental or genetic factors or a combination. It is associated with chromosome 22 deletions and DiGeorge syndrome.
Specific genetic associations include:
Embryology studies show that it is a result of anterior malalignment of the aorticopulmonary septum, resulting in the clinical combination of a VSD, pulmonary stenosis, and an overriding aorta. Right ventricular hypertrophy develops progressively from resistance to blood flow through the right ventricular outflow tract.
Pathophysiology
Four malformations
"Tetralogy" denotes a four-part phenomenon in various fields, including literature, and the four parts the syndrome's name implies are its four signs. This is not to be confused with the similarly named teratology, a field of medicine concerned with abnormal development and congenital malformations, which thereby includes tetralogy of Fallot as part of its subject matter.
As such, by definition, tetralogy of Fallot involves four heart malformations which present together:
| Condition | Description |
|---|---|
| Pulmonary Infundibular Stenosis | A narrowing of the right ventricular outflow tract. It can occur at the pulmonary valve (valvular stenosis) or just below the pulmonary valve (infundibular stenosis). Infundibular pulmonic stenosis is mostly caused by overgrowth of the heart muscle wall (hypertrophy of the septoparietal trabeculae),[15] however the events leading to the formation of the overriding aorta are also believed to be a cause. The pulmonic stenosis is the major cause of the malformations, with the other associated malformations acting as compensatory mechanisms to the pulmonic stenosis.[16] The degree of stenosis varies between individuals with TOF, and is the primary determinant of symptoms and severity. This malformation is infrequently described as sub-pulmonary stenosis or subpulmonary obstruction.[17] |
| Overriding aorta | An aortic valve with biventricular connection, that is, it is situated above the ventricular septal defect and connected to both the right and the left ventricle. The degree to which the aorta is attached to the right ventricle is referred to as its degree of "override." The aortic root can be displaced toward the front (anteriorly) or directly above the septal defect, but it is always abnormally located to the right of the root of the pulmonary artery. The degree of override is extremely variable, with 5-95% of the valve being connected to the right ventricle.[15] |
| Ventricular septal defect (VSD) | A hole between the two bottom chambers (ventricles) of the heart. The defect is centered around the most superior aspect of the ventricular septum (the outlet septum), and in the majority of cases is single and large. In some cases thickening of the septum (septal hypertrophy) can narrow the margins of the defect.[15] |
| Right ventricular hypertrophy | The right ventricle is more muscular than normal, causing a characteristic boot-shaped (coeur-en-sabot) appearance as seen by chest X-ray. Due to the misarrangement of the external ventricular septum, the right ventricular wall increases in size to deal with the increased obstruction to the right outflow tract. This feature is now generally agreed to be a secondary anomaly, as the level of hypertrophy tends to increase with age.[18] |
There is anatomic variation between the hearts of individuals with tetralogy of Fallot. Primarily, the degree of right ventricular outflow tract obstruction varies between patients and generally determines clinical symptoms and disease progression.
Presumably, this arises from an unequal growth of the aorticopulmonary septum. The aorta is too large, thus "overriding," and this "steals" from the pulmonary artery, which is therefore stenosed. This then prevents ventricular wall closure, therefore VSD, and this increases the pressures on the right side, and so the R ventricle becomes bigger to handle the work.
Additional anomalies
In addition, tetralogy of Fallot may present with other anatomical anomalies, including:
- stenosis of the left pulmonary artery, in 40%
- a bicuspid pulmonary valve, in 60%
- right-sided aortic arch, in 25%
- coronary artery anomalies, in 10%
- a patent foramen ovale or atrial septal defect, in which case the syndrome is sometimes called a pentalogy of Fallot[19]
- an atrioventricular septal defect
- partially or totally anomalous pulmonary venous return
- forked ribs and scoliosis
Tetralogy of Fallot with pulmonary atresia (pseudotruncus arteriosus) is a severe variant[20] in which there is complete obstruction (atresia) of the right ventricular outflow tract, causing an absence of the pulmonary trunk during embryonic development. In these individuals, blood shunts completely from the right ventricle to the left where it is pumped only through the aorta. The lungs are perfused via extensive collaterals from the systemic arteries, and sometimes also via the ductus arteriosus.
Diagnosis

Congenital heart defects are now diagnosed with echocardiography, which is quick, involves no radiation, is very specific, and can be done prenatally.
Before more sophisticated techniques became available, chest x-ray was the definitive method of diagnosis. The abnormal "coeur-en-sabot" (boot-like) appearance of a heart with tetralogy of Fallot is classically visible via chest x-ray, although most infants with tetralogy may not show this finding.[21] Absence of interstitial lung markings secondary to pulmonary oligaemia are another classic finding in tetralogy,[22] as is the pulmonary bay sign.
Treatment
Tet spells
Tet spells may be treated with beta-blockers such as propranolol, but acute episodes require rapid intervention with morphine or intranasal fentanyl[23] to reduce ventilatory drive, a vasopressor such as phenylephrine, or norepinephrine to increase systemic vascular resistance, and IV fluids for volume expansion.
Oxygen (100%) may be effective in treating spells because it is a potent pulmonary vasodilator and systemic vasoconstrictor. This allows more blood flow to the lungs by decreasing shunting of deoxygenated blood from the right to left ventricle through the VSD. There are also simple procedures such as squatting and the knee chest position which increase systemic vascular resistance and decrease right-to-left shunting of deoxygenated blood into the systemic circulation.[24]
Palliative surgery
The condition was initially thought untreatable until surgeon Alfred Blalock, cardiologist Helen B. Taussig, and lab assistant Vivien Thomas at Johns Hopkins University developed a palliative surgical procedure, which involved forming a side to end anastomosis between the subclavian artery and the pulmonary artery. This first surgery was depicted in the film Something the Lord Made.[25] It was actually Helen Taussig who convinced Alfred Blalock that the shunt was going to work. This redirected a large portion of the partially oxygenated blood leaving the heart for the body into the lungs, increasing flow through the pulmonary circuit, and greatly relieving symptoms in patients. The first Blalock-Thomas-Taussig shunt surgery was performed on 15-month-old Eileen Saxon on November 29, 1944 with dramatic results.
The Potts shunt[26] and the Waterston-Cooley shunt[27][28] are other shunt procedures which were developed for the same purpose. These are no longer used.
Currently, Blalock-Thomas-Taussig shunts are not normally performed on infants with TOF except for severe variants such as TOF with pulmonary atresia (pseudotruncus arteriosus).
Total surgical repair
The Blalock-Thomas-Taussig procedure, initially the only surgical treatment available for tetralogy of Fallot, was palliative but not curative. The first total repair of tetralogy of Fallot was done by a team led by C. Walton Lillehei at the University of Minnesota in 1954 on an 11-year-old boy.[29] Total repair on infants has had success from 1981, with research indicating that it has a comparatively low mortality rate.[30]
Total repair of tetralogy of Fallot initially carried a high mortality risk. This risk has gone down steadily over the years. Surgery is now often carried out in infants one year of age or younger with less than 5% perioperative mortality. The open-heart surgery is designed (1) to relieve the right ventricular outflow tract stenosis by careful resection of muscle and (2) to repair the VSD with a Gore-Tex patch or a homograft. Additional reparative or reconstructive surgery may be done on patients as required by their particular cardiac anatomy.
Epidemiology
Tetralogy of Fallot occurs approximately 400 times per million live births[31] and accounts for 7 to 10% of all congenital heart abnormalities.
Prognosis
Untreated, tetralogy of Fallot rapidly results in progressive right ventricular hypertrophy due to the increased resistance caused by narrowing of the pulmonary trunk. This progresses to heart failure which begins in the right ventricle and often leads to left heart failure and dilated cardiomyopathy. Mortality rate depends on the severity of the tetralogy of Fallot. If left untreated, TOF carries a 35% mortality rate in the first year of life, and a 50% mortality rate in the first three years of life. Untreated TOF also causes delayed growth and development, including delayed puberty.
Patients who have undergone total surgical repair of tetralogy of Fallot have improved hemodynamics and often have good to excellent cardiac function after the operation with some to no exercise intolerance (New York Heart Association Class I-II). Surgical success and long-term outcome greatly depend on the particular anatomy of the patient and the surgeon's skill and experience with this type of repair.
Ninety percent of patients with total repair as infants develop a progressively leaky pulmonary valve later in adulthood. They require, therefore, follow up in specialized Adult Congenital Heart Disease centres. 55% are present.
Notable cases
- Shaun White,[32] snowboarder and 2006 and 2010 Olympic gold medalist and X Games gold medalist from 2003 to 2013.
- Beau Casson,[33] Australian cricketer
- Dennis McEldowney,[34] New Zealand author and publisher
- Max Page, Volkswagen's "Little Darth Vader" from the 2011 Super Bowl commercial[35]
See also
References
- 1 2 "Fallot's tetralogy". Whonamedit?. Retrieved 2 October 2016.
- 1 2 3 4 5 "What Is Tetralogy of Fallot?". NHLBI. 1 July 2011. Retrieved 2 October 2016.
- ↑ "What Are the Signs and Symptoms of Tetralogy of Fallot?". NHLBI. 1 July 2011. Retrieved 2 October 2016.
- ↑ "What Causes Tetralogy of Fallot?". NHLBI. 1 July 2011. Retrieved 2 October 2016.
- ↑ "How Is Tetralogy of Fallot Treated?". NHLBI. July 1, 2011. Retrieved 2 October 2016.
- 1 2 Warnes, Carole A. (July 2005). "The Adult With Congenital Heart Disease". Journal of the American College of Cardiology. 46 (1): 1–8. doi:10.1016/j.jacc.2005.02.083. PMID 15992627.
- ↑ "Types of Congenital Heart Defects". NHLBI. 1 July 2011. Retrieved 2 October 2016.
- ↑ "Tetralogy of Fallot: Overview - eMedicine". Retrieved 2009-01-02.
- ↑ Murakami T (2002). "Squatting: the hemodynamic change is induced by enhanced aortic wave reflection". Am. J. Hypertens. 15 (11): 986–8. doi:10.1016/S0895-7061(02)03085-6. PMID 12441219.
- ↑ Guntheroth WG, Mortan BC, Mullins GL, Baum D. Am Venous return with knee-chest position and squatting in tetralogy of Fallot. Heart J. 1968 Mar;75(3):313-8.
- ↑ Eldadah ZA, Hamosh A, Biery NJ, et al. (January 2001). "Familial Tetralogy of Fallot caused by mutation in the jagged1 gene". Hum. Mol. Genet. 10 (2): 163–9. doi:10.1093/hmg/10.2.163. PMID 11152664.
- ↑ Goldmuntz E, Geiger E, Benson DW (November 2001). "NKX2.5 mutations in patients with tetralogy of Fallot". Circulation. 104 (21): 2565–8. doi:10.1161/hc4601.098427. PMID 11714651.
- ↑ Pizzuti A, Sarkozy A, Newton AL, et al. (November 2003). "Mutations of ZFPM2/FOG2 gene in sporadic cases of tetralogy of Fallot". Hum. Mutat. 22 (5): 372–7. doi:10.1002/humu.10261. PMID 14517948.
- ↑ Lambrechts D, Devriendt K, Driscoll DA, et al. (June 2005). "Low expression VEGF haplotype increases the risk for tetralogy of Fallot: a family based association study". J. Med. Genet. 42 (6): 519–22. doi:10.1136/jmg.2004.026443. PMC 1736071
 . PMID 15937089.
. PMID 15937089. - 1 2 3 Gatzoulis MA, Webb GD, Daubeney PE. (2005) Diagnosis and Management of Adult Congenital Heart Disease. Churchill Livingstone, Philadelphia. ISBN 0-443-07103-9.
- ↑ Bartelings M, Gittenberger-de Groot A (1991). "Morphogenetic considerations on congenital malformations of the outflow tract. Part 1: Common arterial trunk and tetralogy of Fallot". Int. J. Cardiol. 32 (2): 213–30. doi:10.1016/0167-5273(91)90329-N. PMID 1917172.
- ↑ Anderson RH, Weinberg. The clinical anatomy of tetralogy of Fallot. Cardiol Young. 2005 15;38-47. PMID 15934690.
- ↑ Anderson RH, Tynan M. Tetralogy of Fallot – a centennial review. Int J Cardiol. 1988 21; 219-232. PMID 3068155.
- ↑ Cheng TO (1995). "Pentalogy of Cantrell vs pentalogy of Fallot". Tex Heart Inst J. 22 (1): 111–2. PMC 325224. PMID 7787464.
- ↑ Farouk A, Zahka K, Siwik E, et al. (December 2008). "Individualized approach to the surgical treatment of tetralogy of Fallot with pulmonary atresia". Cardiol Young. 19 (1): 1–10. doi:10.1017/S1047951108003430. PMID 19079949.
- ↑ http://radiopaedia.org/articles/tetralogy-of-fallot
- ↑ http://www.scribd.com/shawn_robinson_2/d/74194438/67-Tetralogy-of-Fallot p290
- ↑ Tsze DS, Vitberg YM, Berezow J, Starc TJ, Dayan PS (2014). "Treatment of tetralogy of fallot hypoxic spell with intranasal fentanyl". Pediatrics. 134 (1): e266–9. doi:10.1542/peds.2013-3183. PMID 24936003.
- ↑ Murakami T (2002). "Squatting: the hemodynamic change is induced by enhanced aortic wave reflection". Am. J. Hypertens. 15 (11): 986–8. doi:10.1016/S0895-7061(02)03085-6. PMID 12441219.
- ↑ "First Operations; Blalock - Taussig Shunt". Retrieved 2007-11-15.
- ↑ Boshoff D, Budts W, Daenen W, Gewillig M (January 2005). "Transcatheter closure of a Potts' shunt with subsequent surgical repair of tetralogy of fallot". Catheter Cardiovasc Interv. 64 (1): 121–3. doi:10.1002/ccd.20247. PMID 15619282.
- ↑ Daehnert I, Wiener M, Kostelka M (May 2005). "Covered stent treatment of right pulmonary artery stenosis and Waterston shunt". Ann. Thorac. Surg. 79 (5): 1754–5. doi:10.1016/j.athoracsur.2003.11.059. PMID 15854971.
- ↑ "Systemic to Pulmonary Artery Shunting for Palliation: - eMedicine". Retrieved 2009-01-02.
- ↑ Lillehei CW; Cohen, M; Warden, HE; Read, RC; Aust, JB; Dewall, RA; Varco, RL (1955). "Direct Vision Intracardiac Surgical Correction of the Tetralogy of Fallot, Pentalogy of Fallot, and Pulmonary Atresia Defects Report of First Ten Cases". Ann. Surg. 142 (3): 418–442. doi:10.1097/00000658-195509000-00010. PMC 1465089. PMID 13249340.
- ↑ "Total correction of tetralogy of fallot in the first year of life: late results"..
- ↑ Child JS (July 2004). "Fallot's tetralogy and pregnancy: prognostication and prophesy". J. Am. Coll. Cardiol. 44 (1): 181–3. doi:10.1016/j.jacc.2004.04.009. PMID 15234430.
- ↑ "SI.com - SI Adventure - Double Ripper - Wednesday July 02, 2003 05:14 PM". CNN. Retrieved 2009-01-02.
- ↑ "New twist in Casson's amazing journey - Cricket - Sport - smh.com.au". The Sydney Morning Herald. 2008-06-06. Retrieved 2009-01-02.
- ↑ http://www.bookcouncil.org.nz/writers/mceldowney.html
- ↑ http://www.msnbc.msn.com/id/41455377/ns/business-business_of_super_bowl_xlv/
External links
- What Is Tetralogy of Fallot? at National Institute of Health
- Understanding your child’s heart: Tetralogy of Fallot; by the British Heart Foundation
- Interactive 3-D Animation of Tetralogy of Fallot Repair - Stanford Children's Health