Cataract surgery
| Cataract surgery | |
|---|---|
| Intervention | |
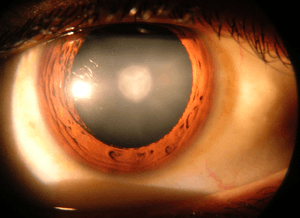 Magnified view of a cataract in a human eye seen on examination with a slit lamp | |
| ICD-9-CM | 13.19 |
| MeSH | D002387 |
| MedlinePlus | 002957 |
Cataract surgery is the removal of the natural lens of the eye (also called "crystalline lens") that has developed an opacification, which is referred to as a cataract. Metabolic changes of the crystalline lens fibers over time lead to the development of the cataract and loss of transparency, causing impairment or loss of vision. Many patients' first symptoms are strong glare from lights and small light sources at night, along with reduced acuity at low light levels. During cataract surgery, a patient's cloudy natural cataract lens is removed and replaced with a synthetic lens to restore the lens's transparency.[1]
Following surgical removal of the natural lens, an artificial intraocular lens implant is inserted (eye surgeons say that the lens is "implanted"). Cataract surgery is generally performed by an ophthalmologist (eye surgeon) in an ambulatory (rather than inpatient) setting, in a surgical center or hospital, using local anesthesia (either topical, peribulbar, or retrobulbar), usually causing little or no discomfort to the patient. Well over 90% of operations are successful in restoring useful vision, with a low complication rate.[2] Day care, high volume, minimally invasive, small incision phacoemulsification with quick post-op recovery has become the standard of care in cataract surgery all over the world.
Types
Two main types of surgical procedures are in common use throughout the world. The first procedure is phacoemulsification (phaco) and the second involves two different types of extracapsular cataract extraction (ECCE). In most surgeries an intraocular lens is inserted. Foldable lenses are generally used for the 2-3mm phaco incision, while non-foldable lenses are placed through the larger extracapsular incision. The small incision size used in phacoemulsification (2-3mm) often allows "sutureless" incision closure. ECCE utilises a larger incision (10-12mm) and therefore usually requires stitching, and this in part led to the modification of ECCE known as manual small incision cataract surgery (MSICS).
Cataract extraction using intracapsular cataract extraction (ICCE) has been superseded by phaco & ECCE, and is rarely performed.
Phacoemulsification is the most commonly performed cataract procedure in the developed world. However, the high cost of a phacoemulsification machine and of the associated disposable equipment means that ECCE and MSICS remain the most commonly performed procedure in developing countries.
Types of surgery


There are a number of different surgical techniques used in cataract surgery:
- Phacoemulsification (phaco) is the most common technique used by developed countries. It involves the use of a machine with an ultrasonic handpiece equipped with a titanium or steel tip. The tip vibrates at ultrasonic frequency (40,000 Hz) and the lens material is emulsified. A second fine instrument (sometimes called a "cracker" or "chopper") may be used from a side port to facilitate cracking or chopping of the nucleus into smaller pieces. Fragmentation into smaller pieces makes emulsification easier, as well as the aspiration of cortical material (soft part of the lens around the nucleus). After phacoemulsification of the lens nucleus and cortical material is completed, a dual irrigation-aspiration (I-A) probe or a bimanual I-A system is used to aspirate out the remaining peripheral cortical material.
- Manual small incision cataract surgery (MSICS): This technique is an evolution of ECCE (see below) where the entire lens is expressed out of the eye through a self-sealing scleral tunnel wound. An appropriately constructed scleral tunnel is watertight and does not require suturing. The "small" in the title refers to the wound being relatively smaller than an ECCE, although it is still markedly larger than a phaco wound. Head to head trials of MSICS vs phaco in dense cataracts have found no difference in outcomes, but shorter operating time and significantly lower costs with MSICS.[3]
- Extracapsular cataract extraction (ECCE): Extracapsular cataract extraction involves the removal of almost the entire natural lens while the elastic lens capsule (posterior capsule) is left intact to allow implantation of an intraocular lens.[4] It involves manual expression of the lens through a large (usually 10–12 mm) incision made in the cornea or sclera. Although it requires a larger incision and the use of stitches, the conventional method may be indicated for patients with very hard cataracts or other situations in which phacoemulsification is problematic.[5]
- Intracapsular cataract extraction (ICCE) involves the removal of the lens and the surrounding lens capsule in one piece. The procedure has a relatively high rate of complications due to the large incision required and pressure placed on the vitreous body. It has therefore been largely superseded and is rarely performed in countries where operating microscopes and high-technology equipment are readily available.[4] After lens removal, an artificial plastic lens (an intraocular lens implant) can be placed in either the anterior chamber or sutured into the sulcus.
- Femtosecond laser appears safe but has few benefits over phacoemulsification.[6]
Cryoextraction is a form of ICCE that freezes the lens with a cryogenic substance such as liquid nitrogen.[7] In this technique, the cataract is extracted through use of a cryoextractor — a cryoprobe whose refrigerated tip adheres to and freezes tissue of the lens, permitting its removal. Although it is now used primarily for the removal of subluxated lenses, it was the favored form of cataract extraction from the late 1960s to the early 1980s.[8]
Intraocular lenses
- Intraocular lens implantation: After the removal of the cataract, an intraocular lens (IOL) is usually implanted into the eye, either through a small incision (1.8 mm to 2.8 mm) using a foldable IOL, or through an enlarged incision, using a PMMA (polymethylmethacrylate) lens. The foldable IOL, made of silicone or acrylic material of appropriate power is folded either using a holder/folder, or a proprietary insertion device provided along with the IOL. The lens implanted is inserted through the incision into the capsular bag within the posterior chamber (in-the-bag implantation). Sometimes, a sulcus implantation (in front or on top of the capsular bag but behind the iris) may be required because of posterior capsular tears or because of zonulodialysis. Implantation of posterior chamber IOL (PCIOL) in patients below 1 year of age is controversial due to rapid ocular growth at this age and the excessive amount of inflammation, which may be very difficult to control. Optical correction in these patients without intraocular lens (aphakic) is usually managed with either special contact lenses or glasses. Secondary implantation of IOL (placement of a lens implant as a second operation) may be considered later. New designs of multifocal intraocular lens are now available. These lenses allow focusing of rays from distant as well as near objects, working much like bifocal or trifocal eyeglasses. Preoperative patient selection and good counselling is extremely important to avoid unrealistic expectations and post-operative patient dissatisfaction. Acceptability for these lenses has become better and studies have shown good results in selected patients.
In addition, there is an accommodating lens that was approved by the US FDA in 2003 and made by Eyeonics,[9] now Bausch & Lomb. The Crystalens is on struts and is implanted in the eye's lens capsule, and its design allows the lens' focusing muscles to move it back and forth, giving the patient natural focusing ability.
Artificial intraocular lenses are used to replace the eye's natural lens that is removed during cataract surgery. These lenses have been increasing in popularity since the 1960s, but it was not until 1981 that the first U.S. Food and Drug Administration (FDA) approval for this type of product was issued. The development of intraocular lenses brought about an innovation as patients previously did not have their natural lens replaced and as a result had to wear very thick eyeglasses or some special type of contact lenses. Presently, IOLs are especially designed for patients with different vision problems. The main types of IOLs that now exist are divided into monofocal and multifocal lenses.

The monofocal intraocular lenses are the traditional ones, which may provide vision at one distance only: far, intermediate, or near.[10] Patients who choose these lenses over the more developed types will have to overcome the disadvantage of wearing eyeglasses or contact lenses for reading or using the computer. These intraocular lenses are usually spherical, and they have their surface uniformly curved.
The multifocal intraocular lens is one of the newest types of such lenses. They are often referred to as "premium" lenses because they are multifocal and accommodative and allow the patient to visualize objects at more than one distance, removing the need to wear eyeglasses or contact lenses. Premium intraocular lenses are those used in correcting presbyopia or astigmatism. Premium intraocular lenses are typically not covered by insurance companies as their additional benefits are considered a luxury and not a medical necessity.[10] An accommodative intraocular lens implant has only one focal point, but it acts as if it is a multifocal IOL. The intraocular lens was designed with a hinge similar to the mechanics of the eye's natural lens.[11]
The intraocular lenses used in correcting astigmatism are called toric and have been FDA approved since 1998. The STAAR Surgical Intraocular Lens was the first such lens ever developed in the United States and it may correct up to 3.5 diopters. A different model of toric lenses is created by Alcon and may correct up to 3 diopters of astigmatism. In order to achieve the most benefit from a toric lens, the surgeon must rotate the lens to be on axis with the patient’s astigmatism. Intraoperative wavefront analysis, such as that provided by the ORA System developed by Wavetec Visions Systems, can be used to assist the doctor in toric lens placement and minimize astigmatic errors.[12]
Cataract surgery may be performed to correct vision problems in both eyes, and in these cases, patients are usually advised to consider monovision. This procedure involves inserting in one eye an intraocular lens that provides near vision and in the other eye an IOL that provides distance vision. Although most patients can adjust to having implanted monofocal lenses in both eyes, some cannot and may experience blurred vision at both near and far. IOLs that emphasize distance vision may be mixed with IOLs that emphasize intermediate vision in order to achieve a type of modified monovision. Bausch and Lomb developed in 2004 the first aspheric IOLs which provide better contrast sensitivity by having their periphery flatter than the middle of the lens. However, some cataract surgeons have debated the benefits of aspheric IOLs, because the contrast sensitivity benefit may not last in older patients.[10]
Some of the newly launched IOLs are able to provide ultraviolet and blue light protection. The crystalline lens of the eye filters these potentially harmful rays and many premium IOLs are designed to undertake this task as well. According to a few studies though, these lenses have been associated with a decrease in vision quality.
Another type of intraocular lenses is the light-adjustable one which is still undergoing FDA clinical trials. This particular type of IOLs is implanted in the eye and then treated with light of a certain wavelength in order to alter the curvature of the lens.
In some cases, surgeons may opt for inserting an additional lens over the already implanted one. This type of IOLs procedures are called "piggyback" IOLs and are usually considered an option whenever the lens result of the first implant is not optimal. In such cases, implanting another IOL over the existent one is considered safer than replacing the initial lens. This approach may also be used in patients who need high degrees of vision correction.
No matter which IOL is used, the surgeon will need to select the appropriate power of IOL (much like an eyeglass prescription) to provide the patient with the desired refractive outcome. Traditionally, doctors use preoperative measurements including corneal curvature, axial length, and white to white measurements to estimate the required power of the IOL. These traditional methods include several formulas including Hagis, Hoffer Q, Holladay 1, Holladay 2, and SRK/T to name a few.[13] Refractive results using traditional power calculation formulas leave patients within 0.5D of target (Correlates to 20/25 when targeted for distance) or better in 55% of cases and within 1D (Correlates to 20/40 when targeted for distance) or better in 85% of cases. Recent developments in interoperative wavefront technology such as the ORA System from Wavetec Vision Systems, have demonstrated in studies to provide power calculations that lead to improved outcomes, yielding 80% of patients within 0.5D (20/25 or better).[12]
Statistically, cataract surgery and IOL implantation seem to be procedures with the safest and highest success rates when it comes to eye care. However, as with any other type of surgery, it implies certain risks. The cost is another important aspect of these lenses. Although most insurance companies cover the costs of traditional IOLs, patients may need to pay the price-difference in case they choose more advanced lenses, such as the premium ones.[14]
Preoperative evaluation
An eye examination or pre-operative evaluation by an eye surgeon is necessary to confirm the presence of a cataract and to determine if the patient is a suitable candidate for surgery. The patient must fulfill certain requirements such as:
- The degree of reduction of vision due, at least in large part, to the cataract should be evaluated. While the existence of other sight-threatening diseases, such as age-related macular degeneration or glaucoma, does not preclude cataract surgery, less improvement may be expected in their presence.
- The eyes should have a normal pressure, or any pre-existing glaucoma should be adequately controlled on medications. In cases of uncontrolled glaucoma, a combined cataract-glaucoma procedure (Phaco-trabeculectomy) can be planned and performed.
- The pupil should be adequately dilated using eyedrops; if pharmacologic pupil dilation is inadequate, procedures for mechanical pupillary dilatation may be needed during the surgery.
- The patients with retinal detachment may be scheduled for a combined vitreo-retinal procedure, along with PC-IOL implantation.
- In addition, it has recently been shown that patients taking tamsulosin (Flomax), a common drug for enlarged prostate, are prone to developing a surgical complication known as intraoperative floppy iris syndrome (IFIS), which must be correctly managed to avoid the complication posterior capsule rupture; however, prospective studies have shown that the risk is greatly reduced if the surgeon is informed of the patient's history with the drug beforehand, and has appropriate alternative techniques prepared.[15]
- A Cochrane Review of three randomized clinical trials including over 21,500 cataract surgeries examined whether routine preoperative medical testing resulted in a reduction of adverse events during surgery.[16] Results showed that performing preoperative medical testing did not result in a reduction of risk of intraoperative or postoperative medical adverse events, compared to surgeries with no or limited preoperative testing.[16]
Operation procedures
The surgical procedure in phacoemulsification for removal of cataract involves a number of steps. Each step must be carefully and skillfully performed in order to achieve the desired result. The steps may be described as follows:
- Anaesthesia;
- Exposure of the eyeball using an eyelid speculum;
- Entry into the eye through a minimal incision (corneal or scleral);
- Viscoelastic injection to stabilize the anterior chamber and to help maintain the eye pressurization;
- Capsulorhexis;
- Hydrodissection pie;
- Hydro-delineation;
- Ultrasonic destruction or emulsification of the cataract after nuclear cracking or chopping (if needed), careful aspiration of the remaining lens cortex (outer layer of lens) material from the capsular bag, capsular polishing (if needed);
- Implantation of the, usually foldable, intra-ocular lens (IOL);
- Viscoelastic removal;
- Wound sealing / hydration (if needed).
The pupil is dilated using drops (if the IOL is to be placed behind the iris) to help better visualise the cataract. Pupil-constricting drops are reserved for secondary implantation of the IOL in front of the iris (if the cataract has already been removed without primary IOL implantation). Anesthesia may be placed topically (eyedrops) or via injection next to (peribulbar) or behind (retrobulbar) the eye. Oral or intravenous sedation may also be used to reduce anxiety. General anesthesia is rarely necessary, but may be employed for children and adults with particular medical or psychiatric issues. The operation may occur on a stretcher or a reclining examination chair. The eyelids and surrounding skin will be swabbed with disinfectant. The face is covered with a cloth or sheet, with an opening for the operative eye. The eyelid is held open with a speculum to minimize blinking during surgery. Pain is usually minimal in properly anesthetised eyes, though a pressure sensation and discomfort from the bright operating microscope light is common. The ocular surface is kept moist using sterile saline eyedrops or methylcellulose viscoelastic. The discission into the lens of the eye is performed at or near where the cornea and sclera meet (limbus = corneoscleral junction). Advantages of the smaller incision include use of few or no stitches and shortened recovery time.[4][17]
A capsulotomy (rarely known as cystotomy) is a procedure to open a portion of the lens capsule, using an instrument called a cystotome.[18] An anterior capsulotomy refers to the opening of the front portion of the lens capsule, whereas a posterior capsulotomy refers to the opening of the back portion of the lens capsule. In phacoemulsification, the surgeon performs an anterior continuous curvilinear capsulorhexis, to create a round and smooth opening through which the lens nucleus can be emulsified and the intraocular lens implant inserted.
Following cataract removal (via ECCE or phacoemulsification, as described above), an intraocular lens is usually inserted. After the IOL is inserted, the surgeon checks that the incision does not leak fluid. This is a very important step, since wound leakage increases the risk of unwanted microrganisms' gaining access into the eye and predispose to endophathalmitis. An antibiotic/steroid combination eyedrop is put in and an eye shield may be applied on the operated eye, sometimes supplemented with an eye patch.
Antibiotics may be administered pre-operatively, intra-operatively, and/or post-operatively. Frequently a topical corticosteroid is used in combination with topical antibiotics postoperatively.
Most cataract operations are performed under a local anaesthetic, allowing the patient to go home the same day. The use of an eye patch may be indicated, usually for about some hours, after which the patient is instructed to start using the eyedrops to control the inflammation and the antibiotics that prevent infection. Lens and cataract procedures are commonly done in an outpatient setting; in the United States, 99.9% of lens and cataract procedures were done in an ambulatory setting in 2012.[19]
Occasionally, a peripheral iridectomy may be performed to minimize the risk of pupillary block glaucoma. An opening through the iris can be fashioned manually (surgical iridectomy) or with a laser (called Nd-YAG laser iridotomy). The laser peripheral iridotomy may be performed either prior to or following cataract surgery.
The iridectomy hole is larger when done manually than when performed with a laser. When the manual surgical procedure is performed, some negative side-effects may occur, such as that the opening of the iris can be seen by others (aesthetics), and the light can fall into the eye through the new hole, creating some visual disturbances. In the case of visual disturbances, the eye and brain often learn to compensate and ignore the disturbances over a couple of months. Sometimes the peripheral iris opening can heal, which means that the hole ceases to exist. This is the reason that the surgeon sometimes makes two holes, so that at least one hole is kept open.
After the surgery, the patient is instructed to use anti-inflammatory and antibiotic eye-drops for up to two weeks (depending on the inflammation status of the eye and some other variables). The eye surgeon will judge, based on each patient's idiosyncrasies, the time length to use the eye drops. The eye will be mostly recovered within a week, and complete recovery should be expected in about a month. The patient should not participate in contact/extreme sports until cleared to do so by the eye surgeon.
Complications
Complications after cataract surgery are relatively uncommon.
- PVD — Posterior vitreous detachment does not directly threaten vision. Even so, it is of increasing interest because the interaction between the vitreous body and the retina might play a decisive role in the development of major pathologic vitreoretinal conditions. PVD may be more problematic with younger patients, since many patients older than 60 have already gone through PVD. PVD may be accompanied by peripheral light flashes and increasing numbers of floaters.
- Some people can develop a posterior capsular opacification (PCO, also called an after-cataract). As a physiological change expected after cataract surgery, the posterior capsular cells undergo hyperplasia and cellular migration, showing up as a thickening, opacification and clouding of the posterior lens capsule (which is left behind when the cataract was removed, for placement of the IOL). This may compromise visual acuity and the ophthalmologist can use a device to correct this situation. It can be safely and painlessly corrected using a laser device to make small holes in the posterior lens capsule of the crystalline. It usually is a quick outpatient procedure that uses a Nd-YAG laser (neodymium-yttrium-aluminum-garnet) to disrupt and clear the central portion of the opacified posterior lens capsule (posterior capsulotomy). This creates a clear central visual axis for improving visual acuity.[20] In very thick opacified posterior capsules, a surgical (manual) capsulectomy is the surgical procedure performed. A YAG capsulotomy is, however, a factor which must be taken in consideration in the event of IOL replacement as vitreous can migrate toward the anterior chamber through the opening hitherto occluded by the IOL.
- Posterior capsular tear may be a complication during cataract surgery. The rate of posterior capsular tear among skilled surgeons is around 2% to 5%. It refers to a rupture of the posterior capsule of the natural lens. Surgical management may involve anterior vitrectomy and, occasionally, alternative planning for implanting the intraocular lens, either in the ciliary sulcus, in the anterior chamber (in front of the iris), or, less commonly, sutured to the sclera.
- Retinal detachment is an uncommon complication of cataract surgery, which may occur weeks, months, or even years later.
- Toxic Anterior Segment Syndrome or TASS is a non-infectious inflammatory condition that may occur following cataract surgery. It is usually treated with topical corticosteroids in high dosage and frequency.
- Endophthalmitis is a serious infection of the intraocular tissues, usually following intraocular surgery, or penetrating trauma. There is some concern that the clear cornea incision might predispose to the increase of endophthalmitis but there is no conclusive study to corroborate this suspicion.
- Glaucoma may occur and it may be very difficult to control. It is usually associated with inflammation, specially when little fragments or chunks of the nucleus get access to the vitreous cavity. Some experts recommend early intervention when this condition happens (posterior pars plana vitrectomy). Neovascular glaucoma may occur, specially in diabetic patients. In some patients, the intraocular pressure may remain so high that blindness may ensue.
- Swelling or edema of the central part of the retina, called macula, resulting in macular edema, can occur a few days or weeks after surgery. Most such cases can be successfully treated. Preventative use of nonsteroidal anti-inflammatory drugs has been reported to reduce the risk of macular edema to some extent.[21]
- Other possible complications include: Swelling or edema of the cornea, sometimes associated with cloudy vision, which may be transient or permanent (pseudophakic bullous keratopathy). Displacement or dislocation of the intraocular lens implant may rarely occur. Unplanned high refractive error (either myopic or hypermetropic) may occur due to error in the ultrasonic ecobiometry (measure of the length and the required intra-ocular lens power). Cyanopsia, in which the patient sees everything tinted with blue, often occurs for a few days, weeks or months after removal of a cataract. Floaters commonly appear after surgery.

History
India
The earliest form of cataract surgery, now known as 'couching', was first found in ancient India and then introduced to other countries by the Indian physician Sushruta (ca. 3rd century CE[22][23]), who described it in his work the Compendium of Sushruta or Sushruta Samhita. The Uttaratantra section of the Compendium, chapter 17, verses 55–69, describes an operation in which a curved needle was used to push the opaque phlegmatic matter (kapha in Sanskrit) in the eye out of the way of vision. The phlegm was then blown out of the nose. The eye would later be soaked with warm clarified butter and then bandaged. Here is translation from the original Sanskrit:
- "vv.55-56: Now procedure of surgical operation of ślaiṣmika liṅganāśa (cataract) will be described. It should be taken up (for treatment) if the diseased portion in the pupillary region is not shaped like half moon, sweat drop or pearl: not fixed, uneven and thin in the centre, streaked or variegated and is not found painful or reddish."
- "vv. 57-61ab: In moderate season, after unction and sudation, the patient should be positioned and held firmly while gazing at his nose steadily. Now the wise surgeon leaving two parts of white circle from the black one towards the outer canthus should open his eyes properly free from vascular network and then with a barley-tipped rod-like instrument held firmly in hand with middle, index and thumb fingers should puncture the natural hole-like point with effort and confidence not below, above or in sides. The left eye should be punctured with right hand and vice-versa. When punctured properly a drop of fluid comes out and alsoe there is some typical sound."
- "vv. 61bc-64ab: Just after puncturing, the expert should irrigate the eye with breast-milk and foment it from outside with vāta-[wind-]alleviating tender leaves, irrespective of doṣa [defect] being stable or mobile, holding the instrument properly in position. Then the pupillary circle should be scraped with the tip of the instrument while the patient, closing the nostril of the side opposite to the punctured eye, should blow so that kapha [phlegm] located in the region be eliminated."
- "vv. 64cd-67: When pupillary region becomes clear like cloudless sun and is painless, it should be considered as scraped properly.
- (If doṣa [defect] can't be eliminated or it reappears, puncturing is repeated after unction and sudation.)
- When the sights are seen properly the śalākā [probe] should be removed slowly, eye anointed with ghee and bandaged. Then the patient :should lie down in supine position in a peaceful chamber.
- He should avoid belching, coughing, sneezing, spitting and shaking during the operation and thereafter should observe the restrictions :as after intake of sneha [oil]."
- "v.68: Eye should be washed with vāta-[wind-]alleviating decoctions after every three days and to eliminate fear of (aggravation of ) vāyu [wind], it should also be fomented as mentioned before (from outside and mildly)."
- "v.69: After observing restrictions for ten days in this way, post-operative measures to normalise vision should be employed along with light diet in proper quantity."[24]
The removal of cataract by surgery was also introduced into China from India, and flourished in the Sui (AD 581-618) and Tang dynasties (AD 618-907).[25]
Europe and the Islamic world
The first references to cataract and its treatment Europe are found in 29 AD in De Medicinae, the work of the Latin encyclopedist Aulus Cornelius Celsus, which also describes a couching operation.[26]
Couching continued to be used throughout the Middle Ages and is still used in some parts of Africa and in Yemen.[27][28] However, couching is an ineffective and dangerous method of cataract therapy, and often results in patients remaining blind or with only partially restored vision.[28] For the most part, it has now been replaced by extracapsular cataract surgery and, especially, phacoemulsification.
The lens can also be removed by suction through a hollow instrument. Bronze oral suction instruments have been unearthed that seem to have been used for this method of cataract extraction during the 2nd century AD.[29] Such a procedure was described by the 10th-century Persian physician Muhammad ibn Zakariya al-Razi, who attributed it to Antyllus, a 2nd-century Greek physician. The procedure "required a large incision in the eye, a hollow needle, and an assistant with an extraordinary lung capacity."[30] This suction procedure was also described by the Iraqi ophthalmologist Ammar ibn Ali of Mosul, in his Choice of Eye Diseases, also written in the 10th century.[30] He presented case histories of its use, claiming to have had success with it on a number of patients.[30] Extracting the lens has the benefit of removing the possibility of the lens migrating back into the field of vision.[31] A later variant of the cataract needle in 14th-century Egypt, reported by the oculist Al-Shadhili, used a screw to produce suction. It is not clear, however, how often this method was used as other writers, including Abu al-Qasim al-Zahrawi and Al-Shadhili, showed a lack of experience with this procedure or claimed it was ineffective.[30]
Eighteenth century and later
In 1748, Jacques Daviel was the first modern European physician to successfully extract cataracts from the eye. In America, an early form of surgery known as cataract couching may have been performed in 1611,[32] and cataract extraction was most likely performed by 1784.[33]
In the 1940s Harold Ridley introduced the concept of implantation of the intraocular lens which permitted more efficient and comfortable visual rehabilitation possible after cataract surgery. The implantation of a foldable intraocular lens is the procedure considered the state-of-the-art.
In 1967, Charles Kelman introduced phacoemulsification, a technique that uses ultrasonic waves to emulsify the nucleus of the crystalline lens in order to remove the cataracts without a large incision. This new method of surgery decreased the need for an extended hospital stay and made the surgery ambulatory. Patients who undergo cataract surgery hardly complain of pain or even discomfort during the procedure. However patients who have topical anesthesia, rather than peribulbar block anesthesia, may experience some discomfort.
According to surveys of members of the American Society of Cataract and Refractive Surgery, approximately 2.85 million cataract procedures were performed in the United States during 2004 and 2.79 million in 2005.[34]
In India, modern surgery with intraocular lens insertion in government- and NGO-sponsored Eye Surgical camps has replaced older surgical procedures.
In rare cases, infections have caused blindness among some of the patients in mass free eye camps in India.[35]
See also
References
Notes
- ↑ U.S. News & World Report, December 17, 2007, page 64.
- ↑ University of Illinois Eye Center. "Cataracts." Retrieved August 18, 2006.
- ↑ Ruit, S et al. . A prospective randomized clinical trial of phacoemulsification vs manual sutureless small-incision extracapsular cataract surgery in Nepal. Am J Ophth 2007.
- 1 2 3 Extracapsular Cataract Extraction - Definition, Purpose, Demographics, Description, Diagnosis/preparation, Aftercare, Risks, Normal results, Morbidity and mortality rates, Alternatives Encyclopedia of Surgery: A Guide for Patients and Caregivers
- ↑ http://www.jerrytaneyesurgery.com/cataract-surgery
- ↑ Alió, JL; Abdou, AA; Puente, AA; Zato, MA; Nagy, Z (June 2014). "Femtosecond laser cataract surgery: updates on technologies and outcomes.". Journal of refractive surgery (Thorofare, N.J. : 1995). 30 (6): 420–7. doi:10.3928/1081597x-20140516-01. PMID 24972409.
- ↑ Cryotherapy for cataracts. Encyclopedia of Surgery
- ↑ Meadow, Norman B. Cryotherapy: A fall from grace, but not a crash. Ophthalmology Times. October 15, 2005.
- ↑ New Device Approval - CrystaLens Model AT-45 Accommodating IOL - P030002. U.S. Food and Drug Administration.
- 1 2 3 "Intraocular Lenses (IOLs): Including Premium, Toric & Aspheric Designs". Retrieved 2010-06-18.
- ↑ "Intraocular Lens Implant Types". Retrieved 2010-06-18.
- 1 2 Dan B. Tran, MD (January 2012). "Optimizing Surgical Outcomes With Intraoperative Aberrometry". bmctoday.net. Cataract and Refractive Surgery Today. Retrieved 28 February 2012.
- ↑ "IOL Power Calculation Formulas". doctor-hill.com. East Valley Ophthalmology. Retrieved 28 February 2012.
- ↑ "Cataract Eye Operation". Retrieved 2010-06-18.
- ↑ Charters, Linda Anticipation is key to managing intra-operative floppy iris syndrome. Ophthalmology Times. June 15, 2006.
- 1 2 Keay L, Lindsley K, Tielsch J, Katz J, Schein O (2012). "Routine preoperative medical testing for cataract surgery". Cochrane Database Syst Rev. 3: CD007293. doi:10.1002/14651858.CD007293.pub3. PMID 22419323.
- ↑ Surgery Encyclopedia - Phacoemulsification for cataracts
- ↑ Capsulorhexis using a cystotome needle during cataract surgery
- ↑ Wier LM, Steiner CA, Owens PL (February 2015). "Surgeries in Hospital-Owned Outpatient Facilities, 2012". HCUP Statistical Brief #188. Rockville, MD: Agency for Healthcare Research and Quality.
- ↑ Surgery Encyclopedia - Laser posterior capsulotomy
- ↑ Lim, Blanche X.; Lim, Chris Hl; Lim, Dawn K.; Evans, Jennifer R.; Bunce, Catey; Wormald, Richard. "Prophylactic non-steroidal anti-inflammatory drugs for the prevention of macular oedema after cataract surgery". The Cochrane Database of Systematic Reviews 2016. 11: CD006683. doi:10.1002/14651858.CD006683.pub3. ISSN 1469-493X. PMID 27801522.
- ↑ P. V. Sharma, Sushruta-Samhita (Varanasi: Caukhambha Visvabharati, 2000), vol. 1, p. iv.
- ↑ Meulenbeld, G. Jan (1999–2002). A History of Indian Medical Literature. Groningen: Forsten.
- ↑ Priya Vrat Sharma, Suśruta-Saṃhitā with English translation of text and Ḍalhaṇa's commentary along with critical notes. Vol ĪI (Kalpasthāna and Uttaratantra) (Varanasi, India: Chaukhambha Visvabharati Oriental Publishers & Distributors, 2001), pp. 202–204.
- ↑ Vijaya Deshpande, "Ophthalmic surgery: a chapter in the history of Sino-Indian medical contacts," Bulletin of the School of Oriental and African Studies 63.3(2000): 370-388. See also, Vijaya Deshpande, "Indian influences on early Chinese ophthalmology: glaucoma as a case study," Bulletin of the School of Oriental and African Studies 62.2(1999): 306–322.
- ↑ Cataract history
- ↑ PCLI: Cataract - History
- 1 2 ‘Couching’ for cataracts remains a persistent problem in Yemen, EuroTimes, September 2005, p. 11.
- ↑ Factors influencing the genesis of neurosurgical technology, William C. Bergman, M.D., Raymond A. Schulz, M.Sc., and Deanna S. Davis, M.S., P.A.-C., Neurosurgical Focus 27, #3 (September 2009), E3; doi:10.3171/2009.6.FOCUS09117.
- 1 2 3 4 Savage-Smith Emilie (2000). "The Practice of Surgery in Islamic Lands: Myth and Reality". Social History of Medicine. 13 (2): 307–321 [318–9]. doi:10.1093/shm/13.2.307.
- ↑ Finger, Stanley (1994). Origins of Neuroscience: A History of Explorations Into Brain Function. Oxford University Press. p. 70. ISBN 0-19-514694-8.
- ↑ Leffler CT, Wainsztein RD (2016). "The first cataract surgeons in Latin America (1611-1830)". Clinical Ophthalmology. 2016 (10): 679–94. doi:10.2147/OPTH.S105825. PMC 4841434
 . PMID 27143845.
. PMID 27143845. - ↑ Leffler CT, Schwartz SG, Grzybowski A, Braich PS (2015). "The first cataract surgeons in Anglo-America". Survey of Ophthalmology. 60 (1): 86–92. doi:10.1016/j.survophthal.2014.08.002. PMC 4262555. PMID 25444521.
- ↑ American Academy of Ophthalmology reference
- ↑ India cataracts scandal: Arrests over 'botched' surgery, BBC, 5 December 2014
Bibliography
- Finger, Stanley (2001). Origins of Neuroscience: A History of Explorations Into Brain Function. US: Oxford University Press. ISBN 0-19-514694-8.
- Lade, Arnie & Svoboda, Robert (2000). Chinese Medicine and Ayurveda. Motilal Banarsidass. ISBN 81-208-1472-X.
External links
- Keith P. Thompson (inventor). "Near Vision Accommodating Intraocular Lens with Adjustable Power" (PDF). U.S. patent No. 5,607,472. Archived from the original (PDF) on 2006-09-07. Retrieved 2007-02-04.
- Cataract Surgery — slideshow by The New York Times