Floater
| Floater | |
|---|---|
|
Simulated image of floaters against a blue sky | |
| Classification and external resources | |
| Specialty | Ophthalmology |
| ICD-10 | H43.9 |
| ICD-9-CM | 379.24 |
| DiseasesDB | 31270 |
| MedlinePlus | 002085 |

Floaters are deposits of various size, shape, consistency, refractive index, and motility within the eye's vitreous humour, which is normally transparent.[1][2] At a young age, the vitreous is transparent, but as one ages, imperfections gradually develop. The common type of floater, which is present in most persons' eyes, is due to degenerative changes of the vitreous humour. The perception of floaters is known as myodesopsia,[3] or less commonly as myodaeopsia, myiodeopsia, or myiodesopsia.[1] They are also called Muscae volitantes (Latin: "flying flies"), or mouches volantes (from the French). Floaters are visible because of the shadows they cast on the retina[4] or refraction of the light that passes through them, and can appear alone or together with several others in one's visual field. They may appear as spots, threads, or fragments of cobwebs, which float slowly before the observer's eyes.[2] As these objects exist within the eye itself, they are not optical illusions but are entoptic phenomena. They are not to be confused with visual snow, although these two conditions may co-exist.
Signs and symptoms
 | |
|
|
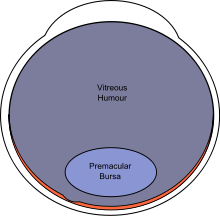
Eye floaters are suspended in the vitreous humour, the thick fluid or gel that fills the eye.[5] The vitreous humour, or vitreous body, is a jelly-like, transparent substance that fills a majority of the eye. It lies within the vitreous chamber behind the lens, and is one of the four optical components of the eye.[6] Thus, floaters follow the rapid motions of the eye, while drifting slowly within the fluid. When they are first noticed, the natural reaction is to attempt to look directly at them. However, attempting to shift one's gaze toward them can be difficult as floaters follow the motion of the eye, remaining to the side of the direction of gaze. Floaters are, in fact, visible only because they do not remain perfectly fixed within the eye. Although the blood vessels of the eye also obstruct light, they are invisible under normal circumstances because they are fixed in location relative to the retina, and the brain "tunes out" stabilized images due to neural adaptation. This stabilization is often interrupted by floaters, especially when they tend to remain visible.[2]
Floaters are particularly noticeable when looking at a blank surface or an open monochromatic space, such as blue sky. Despite the name "floaters", many of these specks have a tendency to sink toward the bottom of the eyeball, in whichever way the eyeball is oriented; the supine position (looking up or lying back) tends to concentrate them near the fovea, which is the center of gaze, while the textureless and evenly lit sky forms an ideal background against which to view them.[5] The brightness of the daytime sky also causes the eyes' pupils to contract, reducing the aperture, which makes floaters less blurry and easier to see.
Floaters present at birth usually remain lifelong, while those that appear later may disappear within weeks or months.[7] They are not uncommon, and do not cause serious problems for most persons; they represent one of the most common presentations to hospital eye services. A survey of optometrists in 2002 suggested that an average of 14 patients per month per optometrist presented with symptoms of floaters in the UK.[8] However, floaters are more than a nuisance and a distraction to those with severe cases, especially if the spots seem to constantly drift through the field of vision. The shapes are shadows projected onto the retina by tiny structures of protein or other cell debris discarded over the years and trapped in the vitreous humour. Floaters can even be seen when the eyes are closed on especially bright days, when sufficient light penetrates the eyelids to cast the shadows. It is not, however, only elderly persons who are troubled by floaters; they can also become a problem to younger people, especially if they are myopic. They are also common after cataract operations or after trauma.
Floaters are able to catch and refract light in ways that somewhat blur vision temporarily until the floater moves to a different area. Often they trick persons who are troubled by floaters into thinking they see something out of the corner of their eye that really is not there. Most persons come to terms with the problem, after a time, and learn to ignore their floaters. For persons with severe floaters it is nearly impossible to completely ignore the large masses that constantly stay within almost direct view.
Floaters have been reported in patients as young as 3. Floaters in teenage patients and young adults are usually harder to treat. For persons in this age group, the floater that is seen usually looks like a kind of translucent worm/web/cell. Very little is known about this region, and it only becomes distinct after the vitreous humour detaches from the retina at later stages of life. Due to their microscopic size they cannot be seen by doctors. They only appear as big as they do because of their proximity to the retina. This type of floater is still described occasionally in people in their 30s and very rarely occurs in people in their 40s.[9][10]
Causes
There are various causes for the appearance of floaters, of which the most common are described here. Simply stated, any damage to the eye that causes material to enter the vitreous humour can result in floaters.
Floaters can be a sign of retinal detachment or a retinal tear but in most cases (98% according to the National Health Service) it is simply age-related or due to natural change in the vitreous humour.
Vitreous syneresis
The most common cause of floaters is shrinkage of the vitreous humour. This gel-like substance consists of 99% water and 1% solid elements. The solid portion consists of a network of collagen and hyaluronic acid, with the latter retaining water molecules. Depolymerization of this network makes the hyaluronic acid release its trapped water, thereby liquefying the gel. The collagen breaks down into fibrils, which ultimately are the floaters that plague the patient. Floaters caused in this way tend to be few in number and of a linear form.
Posterior vitreous detachments and retinal detachments

In time, the liquefied vitreous body loses support and its framework contracts. This leads to posterior vitreous detachment, in which the vitreous membrane is released from the sensory retina. During this detachment, the shrinking vitreous can stimulate the retina mechanically, causing the patient to see random flashes across the visual field, sometimes referred to as "flashers", a symptom more formally referred to as photopsia. The ultimate release of the vitreous around the optic nerve head sometimes makes a large floater appear, usually in the shape of a ring ("Weiss ring").[11] As a complication, part of the retina might be torn off by the departing vitreous membrane, in a process known as retinal detachment. This will often leak blood into the vitreous, which is seen by the patient as a sudden appearance of numerous small dots, moving across the whole field of vision. Retinal detachment requires immediate medical attention, as it can easily cause blindness. Consequently, both the appearance of flashes and the sudden onset of numerous small floaters should be rapidly investigated by an eye care provider.[12]
Regression of the hyaloid artery
The hyaloid artery, an artery running through the vitreous humour during the fetal stage of development, regresses in the third trimester of pregnancy. Its disintegration can sometimes leave cell matter.[13]
Other common causes
Patients with retinal tears may experience floaters if red blood cells are released from leaky blood vessels, and those with uveitis or vitritis, as in toxoplasmosis, may experience multiple floaters and decreased vision due to the accumulation of white blood cells in the vitreous humour.[14]
Other causes for floaters include cystoid macular edema and asteroid hyalosis. The latter is an anomaly of the vitreous humour, whereby calcium clumps attach themselves to the collagen network. The bodies that are formed in this way move slightly with eye movement, but then return to their fixed position.
Tear film debris
Sometimes the appearance of floaters has to be attributed to dark specks in the tear film of the eye. Technically, these are not floaters, but they do look the same from the viewpoint of the patient. Persons with blepharitis or a dysfunctional meibomian gland are especially prone to this cause, but ocular allergies can also cause the problem. To differentiate between material in the vitreous humour of the eye and debris in the tear film, one can look at the effect of blinking: debris in the tear film will move quickly with a blink, while floaters are largely unresponsive to it. Tear film debris is diagnosed by eliminating the possibility of true floaters and macular degeneration.
Diagnosis
Floaters are often readily observed by an ophthalmologist or an optometrist with the use of an ophthalmoscope or slit lamp. However, if the floater is near the retina, it may not be visible to the observer even if it appears large to the sufferer.
Increasing background illumination or using a pinhole to effectively decrease pupil diameter may allow a person to obtain a better view of his or her own floaters. The head may be tilted in such a way that one of the floaters drifts towards the central axis of the eye. In the sharpened image the fibrous elements are more conspicuous.[15]
The presence of retinal tears with new onset of floaters was surprisingly high (14%; 95% confidence interval, 12–16%) as reported in a metaanalysis published as part of the Rational Clinical Examination Series in the Journal of the American Medical Association.[16] Patients with new onset flashes and/or floaters, especially when associated with visual loss or restriction in the visual field, should seek more urgent ophthalmologic evaluation.
Treatment
While surgeries do exist to correct for severe cases of floaters, there are currently no medications (including eye drops) that can correct for this vitreous deterioration. Floaters are often caused by the normal aging process and will usually disappear as the brain learns to ignore them. Looking up/down and left/right will cause the floaters to leave the direct field of vision as the vitreous humour swirls around due to the sudden movement.[17] If floaters significantly increase in numbers and/or severely affect vision, then one of the below surgeries may be necessary.
Currently, insufficient evidence is available to compare the efficacy of surgical vitrectomy with laser vitreolysis the treatment of floaters. A protocol for a Cochrane meta-analysis has been established, in anticipation of relevant randomized controlled trials in the future.[18]
Aggressive marketing campaigns are currently promoting the use of laser vitreolysis for the treatment of floaters.[19][20] No strong evidence currently exists for the treatment of floaters with laser vitreolysis. Currently, the strongest available evidence comparing these two treatment modalities are retrospective case series.[21]
Surgery
Vitrectomy may be successful in treating more severe cases.[22][23] The technique usually involves making three openings through the part of the sclera known as the pars plana. Of these small gauge instruments, one is an infusion port to resupply a saline solution and maintain the pressure of the eye, the second is a fiber optic light source, and the third is a vitrector. The vitrector has a reciprocating cutting tip attached to a suction device. This design reduces traction on the retina via the vitreous material. A variant sutureless, self-sealing technique is sometimes used.
Like most invasive surgical procedures, however, vitrectomy carries a risk of complications,[24] including: retinal detachment, anterior vitreous detachment and macular edema – which can threaten vision or worsen existing floaters (in the case of retinal detachment).
Laser
Laser vitreolysis is a possible treatment option for the removal of vitreous strands and opacities (floaters). In this procedure an ophthalmic laser (usually a yttrium aluminium garnet "YAG" laser) applies a series of nanosecond pulses of low-energy laser light to evaporate the vitreous opacities and to sever the vitreous strands. During this process, the laser energy evaporates the collagen and hyaluronin molecules to form a gas. (It is important to note that the laser energy applied during vitreolysis treatment does not simply break the floater into smaller pieces. Instead, the laser energy converts the floater material to a gas, which is then absorbed into the eye.) The end result is that the floater is removed and/or reduced to a size that no longer impedes vision.
Vitreolysis is an outpatient procedure, which is much less invasive to the eye than a vitrectomy. Side effects may include cataract and intraocular pressure (IOP) spike. Highly effective, it offers a very good degree of patient satisfaction. It can also delay or obviate surgery.
The technique of using YAG lasers to treat vitreous strands and opacities dates to the 1980s, when professors Aron Rosa (Paris, France) and Franz Fankhauser (Berne, Switzerland), pioneers in the use of YAG lasers, both published on their success with vitreolysis.
In a Dutch study by Cees van der Windt, MD, and colleagues, 100 eyes, with PVD-related floaters persisting for more than nine months, were treated with YAG laser vitreolysis (n = 65) or pars plana vitrectomy (n = 35).[25] After all eyes were treated, both the YAG and vitrectomy groups reported an improvement in vision at 85% and 90% respectively. Furthermore, over a follow-up period of eight years, no complications were observed among YAG-treated patients. These findings support those of two small-scale 1990s studies conducted by Tsai, et al., and Toczolowski, et al.. In both studies, a near 100% rate of floater removal was achieved with Nd:YAG laser vitreolysis, and no intra- or post-operative complications occurred in any patient.
The number of floaters treated during a treatment session depends on the type of floater(s) and the laser energy required to treat the floater(s) (that is, to convert the floater material into a gas). During treatment, the ophthalmologist will monitor the level of laser energy used for each shot, as well as the total amount of energy delivered to the eye. In order to ensure safe, effective treatment with minimal patient discomfort, if these energy levels fall outside a predetermined range then any remaining floaters will need to be treated in a subsequent treatment session.
On average, most patients can expect a 60–90% improvement in the mass and/or number of floaters following treatment with vitreolysis. Every eye is different and there are a number of variables that affect the outcome of treatment. Some floaters, for example, are located too close to the retina and cannot be safely treated. The majority of patients will need to undergo two or three treatment sessions in order to achieve a satisfactory result.
When performed with a YAG laser designed specifically for vitreolysis, reported side effects and complications associated with vitreolysis are rare. However, YAG lasers have traditionally been designed for use in the anterior portion of the eye, i.e. posterior capsulotomy and iridotomy treatments. As a result, they often provide a limited view of the vitreous, which can make it difficult to identify the targeted floaters and membranes. They also carry a high risk of damage to surrounding ocular tissue. Accordingly, vitreolysis is not widely practised, being performed by very few specialists. One of them, John Karickhoff, has performed the procedure more than 1,400 times and claims a 90 percent success rate.[26] However, the MedicineNet web site states that "there is no evidence that this [laser treatment] is effective. The use of a laser also poses significant risks to the vision in what is otherwise a healthy eye."[27] A YAG laser optimized for use in the posterior segment, in addition to use in the anterior segment, is recommended for vitreolysis. In order to visualize the floater and target accordingly, the laser's light source must be positioned in the same optical axis as the ophthalmologist's visual axis. Most conventional YAG lasers, in contrast, use a lower angle of illuminating light. Whilst these lasers are well-suited to use in the anterior part of the eye, they are ill-equipped for use in the vitreous chamber, and thereby make it difficult for the ophthalmologist to visualize (and treat) the floater(s).
Medication
Enzymatic vitreolysis has been trialled to treat vitreomacular traction (VMT) and anomalous posterior vitreous detachment. Whilst the mechanism of action may have an effect on clinically significant floaters, as of March 2015 there are no clinical trials being undertaken to determine whether this may be a therapeutic alternative to either i) conservative management, or ii) vitrectomy.[28]
See also
- Blue field entoptic phenomenon, alias Scheerer's phenomenon – tiny bright dots moving quickly in the visual field.
- Distorted vision
- Phosphene
- Synchysis scintillans
- Scotoma
- Ocular straylight
References
- 1 2 Cline D; Hofstetter HW; Griffin JR. Dictionary of Visual Science. 4th ed. Butterworth-Heinemann, Boston 1997. ISBN 0-7506-9895-0
- 1 2 3 "Facts about floaters". National Eye Institute. December 2007. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ From Greek μυιώδης "fly-like" (Myiodes was also the name of a fly-deterring deity) and ὄψις "sight."
- ↑ American Academy of Ophthalmology. "Floaters and Flashes: A Closer Look" (pamphlet) San Francisco: AAO, 2006. ISBN 1-56055-371-5
- 1 2 "Eye floaters and spots; Floaters or spots in the eye". National Eye Institute. Archived from the original on October 23, 2007. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ Saladin, Kenneth (2012). Aanatomy & Physiology: A Unity of Form and Function. New York: McGraw-Hill. p. 614. ISBN 978-0-07-337825-1.
- ↑ "Floaters may remain indefinitely". Archived from the original on September 24, 2015.
- ↑ Craig Goldsmith; Tristan McMullan; Ted Burton (2007). "Floaterectomy Versus Conventional Pars Plana Vitrectomy For Vitreous Floaters". Digital Journal of Ophthalmology. Retrieved 2008-04-11.
- ↑ "Age 30 and Younger". South Florida Eye Foundation. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ "Who can we help?". Vitreous Floater Solutions. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ "Flashes & Floaters". The Eye Digest. Retrieved 2008-02-24.
- ↑ "Flashes and Floaters (Posterior Vitreous Detachment)". St. Luke's Cataract & Laser Institute. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ Floaters in fetal development Archived December 26, 2008, at the Wayback Machine.
- ↑ Alan G. Kabat; Joseph W. Sowka (April 2009). "A clinician's guide to flashes and floaters" (PDF). optometry.co.uk. Retrieved 2008-04-10.
- ↑ Judith Lee, and Gretchyn Bailey;; Dr. Vance Thompson. "Eye floaters and spots". All about vision. Retrieved February 2008. Check date values in:
|access-date=(help) - ↑ Hollands H, Johnson D, Brox AC, Almeida D, Simel DL, Sharma S. Acute-onset floaters and flashes: is this patient at risk for retinal detachment? JAMA. 2009 November 25;302(20):2243–9.
- ↑ "Flashes and Floaters" (PDF). National Library of Medicine. Archived from the original (PDF) on July 28, 2013. Retrieved 9 December 2013.
- ↑ "Laser or vitrectomy for vitreous floaters". wiley.com.
- ↑ "Archived copy". Archived from the original on 2016-05-01. Retrieved 2016-04-11.
- ↑ "Archived copy". Archived from the original on 2016-05-02. Retrieved 2016-04-11.
- ↑ Delaney YM, Oyinloye A, Benjamin L (January 2002). "Nd:YAG vitreolysis and pars plana vitrectomy: surgical treatment for vitreous floaters". Eye (Lond). 16: 21–6. doi:10.1038/sj.eye.6700026. PMID 11913884.
- ↑ Roth M, Trittibach P, Koerner F, Sarra G (Sep 2005). "[Pars plana vitrectomy for idiopathic vitreous floaters.]". Klin Monatsbl Augenheilkd. 222 (9): 728–32. doi:10.1055/s-2005-858497. PMID 16175483.
- ↑ %5b%5bCategory:All articles with dead external links%5d%5d%5b%5bCategory:Articles with dead external links from June 2011%5d%5d "Pars plana vitrectomy (PPV) & floater only vitrectomy" Check
|url=value (help). Retrieved February 2008. Check date values in:|access-date=(help) - ↑ "Facts About Floaters". nih.gov.
- ↑ "www.ellex.de" (PDF). ellex.de.
- ↑ "Surgery To Rid Eye "Floaters" Scrutinized". CBSNews HealthWatch. Retrieved December 5, 2011.
- ↑ "Eye Floaters". MedicineNet. Retrieved December 5, 2011.
- ↑ "Pharmacologic vitreolysis". One Clear Vision.
External links
- What are Floaters Educational Video
- Eye Floaters Simulator
- Diagram of Eye Floaters an entoptic subjective visual phenomena
- Eye Floaters, Flashes and Spots, by Marilyn Haddrill, All About Vision
- Picture of the entoptic phenomenon: Vitreous Floaters
- Video describing history and science of seeing floaters