Placenta
| placenta | |
|---|---|
 Placenta | |
 Human placenta from just after birth with the umbilical cord in place | |
| Details | |
| Precursor | decidua basalis, chorion frondosum |
| Identifiers | |
| Latin | Placento |
| Code | TE E5.11.3.1.1.0.5 |
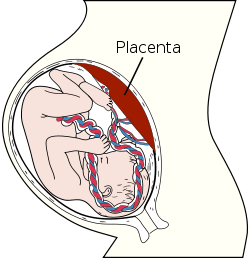
The placenta (also known as afterbirth) is an organ that connects the developing fetus to the uterine wall to allow nutrient uptake, provide thermo-regulation to the fetus, waste elimination, and gas exchange via the mother's blood supply, fight against internal infection and produce hormones to support pregnancy. The placenta provides oxygen and nutrients to growing babies and removes waste products from the baby's blood. The placenta attaches to the wall of the uterus, and the baby's umbilical cord develops from the placenta. The umbilical cord is what connects the mother and the baby. Placentas are a defining characteristic of placental mammals, but are also found in some non-mammals with varying levels of development.[1] The homology of such structures in various viviparous organisms is debatable and, in invertebrates such as Arthropoda, is analogous at best.
The word placenta comes from the Latin word for cake, from Greek πλακόεντα/πλακοῦντα plakóenta/plakoúnta, accusative of πλακόεις/πλακούς plakóeis/plakoús, "flat, slab-like",[2][3] in reference to its round, flat appearance in humans. The classical plural is placentae, but the form placentas is common in modern English and probably has the wider currency at present.
Prototherial (egg-laying) and metatherial (marsupial) mammals produce a choriovitelline placenta that, while connected to the uterine wall, provides nutrients mainly derived from the egg sac.
The placenta functions as a fetomaternal organ with two components: the fetal placenta (Chorion frondosum), which develops from the same blastocyst that forms the fetus, and the maternal placenta (Decidua basalis), which develops from the maternal uterine tissue.[4]
Structure
In humans, the placenta averages 22 cm (9 inch) in length and 2–2.5 cm (0.8–1 inch) in thickness, with the center being the thickest, and the edges being the thinnest. It typically weighs approximately 500 grams (just over 1 lb). It has a dark reddish-blue or crimson color. It connects to the fetus by an umbilical cord of approximately 55–60 cm (22–24 inch) in length, which contains two umbilical arteries and one umbilical vein.[5] The umbilical cord inserts into the chorionic plate (has an eccentric attachment). Vessels branch out over the surface of the placenta and further divide to form a network covered by a thin layer of cells. This results in the formation of villous tree structures. On the maternal side, these villous tree structures are grouped into lobules called cotyledons. In humans, the placenta usually has a disc shape, but size varies vastly between different mammalian species.[6]
Microbiota
The healthy placenta was considered to be a sterile organ but studies published in 2013 and 2014 showed that the placenta is a niche of the human microbiome, and those studies provided initial characterization of the placental flora;[7][8] these microorganisms are distinct from viruses, fungi, and bacteria that cause infection and preterm birth in chorioamnionitis and other pregnancy complications.[7] While biofilms are often found in the amniotic fluid of failed pregnancies, they are found in particulate matter that is found in about 1% of health pregnancies; as of 2015 it was not known whether these biofilms are part of the normal placental flora.[8]
The placental flora more closely resembles that of the oral microbiome than either the vaginal or rectal microbiome; the reason why was not known as of 2015.[7]
In non-human animals, part of the microbiome is passed onto offspring even before the offspring are born. Bacteriologists assume that the same probably holds true for humans.[8]
Physiology
Development

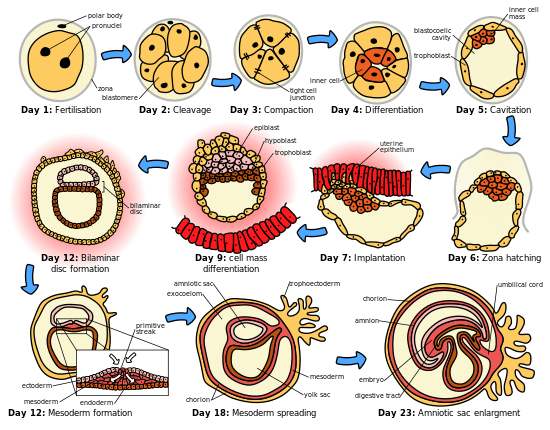
The placenta begins to develop upon implantation of the blastocyst into the maternal endometrium. The outer layer of the blastocyst becomes the trophoblast, which forms the outer layer of the placenta. This outer layer is divided into two further layers: the underlying cytotrophoblast layer and the overlying syncytiotrophoblast layer. The syncytiotrophoblast is a multinucleated continuous cell layer that covers the surface of the placenta. It forms as a result of differentiation and fusion of the underlying cytotrophoblast cells, a process that continues throughout placental development. The syncytiotrophoblast (otherwise known as syncytium), thereby contributes to the barrier function of the placenta.
The placenta grows throughout pregnancy. Development of the maternal blood supply to the placenta is complete by the end of the first trimester of pregnancy (approximately 12–13 weeks).
Placental circulation
Maternal placental circulation
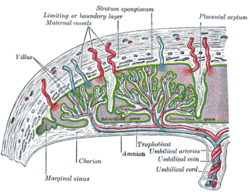
In preparation for implantation of the blastocyst, the uterine endometrium undergoes "decidualisation". Spiral arteries in decidua are remodeled so that they become less convoluted and their diameter is increased. The increased diameter and straighter flow path both act to increase maternal blood flow to the placenta. The relatively high pressure as the maternal blood fills intervillous space through these spiral arteries bathes the fetal villi in blood, allowing an exchange of gases to take place. In humans and other hemochorial placentals, the maternal blood comes into direct contact with the fetal chorion, though no fluid is exchanged. As the pressure decreases between pulses, the deoxygenated blood flows back through the endometrial veins.
Maternal blood flow is approximately 600–700 ml/min at term.
Fetoplacental circulation
Deoxygenated fetal blood passes through umbilical arteries to the placenta. At the junction of umbilical cord and placenta, the umbilical arteries branch radially to form chorionic arteries. Chorionic arteries, in turn, branch into cotyledon arteries. In the villi, these vessels eventually branch to form an extensive arterio-capillary-venous system, bringing the fetal blood extremely close to the maternal blood; but no intermingling of fetal and maternal blood occurs ("placental barrier").[9]
Endothelin and prostanoids cause vasoconstriction in placental arteries, while nitric oxide causes vasodilation.[10] On the other hand, there is no neural vascular regulation, and catecholamines have only little effect.[10]
The fetoplacental circulation is vulnerable to persistent hypoxia or intermittent hypoxia and reoxygenation, which can lead to generation of excessive free radicals. This may contribute to pre-eclampsia and other pregnancy complications.[11] It is proposed that melatonin plays a role as an antioxidant in the placenta.[11]
Birth
Placental expulsion begins as a physiological separation from the wall of the uterus. The period from just after the child is born until just after the placenta is expelled is called the "third stage of labor". The placenta is usually expelled within 15–30 minutes of birth.
Placental expulsion can be managed actively, for example by giving oxytocin via intramuscular injection followed by cord traction to assist in delivering the placenta. Alternatively, it can be managed expectantly, allowing the placenta to be expelled without medical assistance. A Cochrane study suggests that blood loss and the risk of postpartum bleeding will be reduced in women offered active management of the third stage of labour.[12]
The habit is to cut the cord immediately after birth, but allegedly there is no medical reason to do that; on the contrary, it is theorized that not cutting the cord helps the baby in its adaptation to extrauterine life, especially in preterm infants.[13]
Functions
Nutrition

The perfusion of the intervillous spaces of the placenta with maternal blood allows the transfer of nutrients and oxygen from the mother to the fetus and the transfer of waste products and carbon dioxide back from the fetus to the maternal blood supply. Nutrient transfer to the fetus occurs via both active and passive transport. Active transport systems allow significantly different plasma concentrations of various large molecules to be maintained on the maternal and fetal sides of the placental barrier.[14] Adverse pregnancy situations, such as those involving maternal diabetes or obesity, can increase or decrease levels of nutrient transporters in the placenta resulting in overgrowth or restricted growth of the fetus.[15]
Excretion
Waste products excreted from the fetus such as urea, uric acid, and creatinine are transferred to the maternal blood by diffusion across the placenta.
Immunity
IgG antibodies can pass through the human placenta, thereby providing protection to the fetus in utero.[16] This transfer of antibodies begins as early as the 20th week of gestational age, and certainly by the 24th week.[17] This passive immunity lingers for several months after birth, thus providing the newborn with a carbon copy of the mother's long-term humoral immunity to see the infant through the crucial first months of extrauterine life. IgM, however, cannot cross the placenta, which is why some infections acquired during pregnancy can be hazardous for the fetus.
Furthermore, the placenta functions as a selective maternal-fetal barrier against transmission of microbes. However, insufficiency in this function may still cause mother-to-child transmission of infectious diseases.
Endocrine function
- The first hormone released by the placenta is called the human chorionic gonadotropin hormone. This is responsible for stopping the process at the end of menses when the Corpus luteum ceases activity and atrophies. If hCG did not interrupt this process, it would lead to spontaneous abortion of the fetus. The corpus luteum also produces and releases progesterone and estrogen, and hCG stimulates it to increase the amount that it releases. hCG is also what is the indicator of pregnancy, and the hormone that pregnancy tests look for. These tests will work when menses has not occurred or after implantation has happened on days seven to ten. hCG may also have an anti-antibody effect, protecting it from being rejected by the mother’s body. hCG also assists the male fetus by stimulating the testes to produce testosterone, which is the hormone needed to allow the sex organs of the male to grow.
- Progesterone helps the embryo implant by assisting passage through the fallopian tubes. It also affects the fallopian tubes and the uterus by stimulating an increase in secretions necessary for fetal nutrition. Progesterone, like hCG, is necessary to prevent spontaneous abortion because it prevents contractions of the uterus, and is necessary for implantation.
- Estrogen is a crucial hormone in the process of proliferation. This involves the enlargement of the breasts and uterus, allowing for growth of the fetus and production of milk. Estrogen is also responsible for increased blood supply towards the end of pregnancy through vasodilation. The levels of estrogen during pregnancy can increase so that they are thirty times what a non-pregnant woman mid-cycles estrogen level would be.
- Human placental lactogen is a hormone used in pregnancy to develop fetal metabolism and general growth and development. Human placental lactogen works with Growth hormone to stimulate Insulin-like growth factor production and regulating intermediary metabolism. In the fetus, hPL acts on lactogenic receptors to modulate embryonic development, metabolism and stimulate production of IGF, insulin, surfactant and adrenocortical hormones. hPL values increase with multiple pregnancies, intact molar pregnancy, diabetes and Rh incompatibility. They are decreased with toxemia, choriocarcinoma, and Placental insufficiency.[18][19]
Cloaking from immune system of mother
The placenta and fetus may be regarded as a foreign allograft inside the mother, and thus must evade from attack by the mother's immune system.
For this purpose, the placenta uses several mechanisms:
- It secretes Neurokinin B-containing phosphocholine molecules. This is the same mechanism used by parasitic nematodes to avoid detection by the immune system of their host.[20]
- There is presence of small lymphocytic suppressor cells in the fetus that inhibit maternal cytotoxic T cells by inhibiting the response to interleukin 2.[21]
However, the Placental barrier is not the sole means to evade the immune system, as foreign fetal cells also persist in the maternal circulation, on the other side of the placental barrier.[22]
Other functions
The placenta also provides a reservoir of blood for the fetus, delivering blood to it in case of hypotension and vice versa, comparable to a capacitor.[23]

Clinical significance

Numerous pathologies can affect the placenta.
- Placenta accreta, when the placenta implants too deeply, all the way to the actual muscle of uterine wall (without penetrating it)
- Placenta praevia, when the placement of the placenta is too close to or blocks the cervix
- Placental abruption/abruptio placentae
Infections involving the placenta:
- Placentitis, such as the TORCH infections.
- Chorioamnionitis.
Society and culture
The placenta often plays an important role in various cultures, with many societies conducting rituals regarding its disposal. In the Western world, the placenta is most often incinerated.[24]
Some cultures bury the placenta for various reasons. The Māori of New Zealand traditionally bury the placenta from a newborn child to emphasize the relationship between humans and the earth.[25] Likewise, the Navajo bury the placenta and umbilical cord at a specially chosen site,[26] particularly if the baby dies during birth.[27] In Cambodia and Costa Rica, burial of the placenta is believed to protect and ensure the health of the baby and the mother.[28] If a mother dies in childbirth, the Aymara of Bolivia bury the placenta in a secret place so that the mother's spirit will not return to claim her baby's life.[29]
The placenta is believed by some communities to have power over the lives of the baby or its parents. The Kwakiutl of British Columbia bury girls' placentas to give the girl skill in digging clams, and expose boys' placentas to ravens to encourage future prophetic visions. In Turkey, the proper disposal of the placenta and umbilical cord is believed to promote devoutness in the child later in life. In Ukraine, Transylvania, and Japan, interaction with a disposed placenta is thought to influence the parents' future fertility.
Several cultures believe the placenta to be or have been alive, often a relative of the baby. Nepalese think of the placenta as a friend of the baby; Malaysian Orang Asli regard it as the baby's older sibling. The Igbo of Nigeria consider the placenta the deceased twin of the baby, and conduct full funeral rites for it.[28] Native Hawaiians believe that the placenta is a part of the baby, and traditionally plant it with a tree that can then grow alongside the child.[24] Various cultures in Indonesia, such as Javanese, believe that the placenta has a spirit and needs to be buried outside the family house.
In some cultures, the placenta is eaten, a practice known as placentophagy. In some eastern cultures, such as China, the dried placenta (ziheche 紫河車, literally "purple river cart") is thought to be a healthful restorative and is sometimes used in preparations of traditional Chinese medicine and various health products.[30] The practice of human placentophagy has become a more recent trend in western cultures and is not without controversy; its practice being considered cannibalism is debated.
Some cultures have alternative uses for placenta that include the manufacturing of cosmetics, pharmaceuticals and food.
Additional images
 Fetus of about 8 weeks, enclosed in the amnion. Magnified a little over two diameters.
Fetus of about 8 weeks, enclosed in the amnion. Magnified a little over two diameters. Picture of freshly delivered placenta and umbilical cord wrapped around Kelly clamps
Picture of freshly delivered placenta and umbilical cord wrapped around Kelly clamps Fresh human placenta
Fresh human placenta
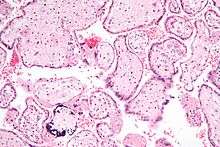 Micrograph of CMV placentitis.
Micrograph of CMV placentitis. A 3D Power doppler image of vasculature in 20-week placenta
A 3D Power doppler image of vasculature in 20-week placenta Placenta held.
Placenta held.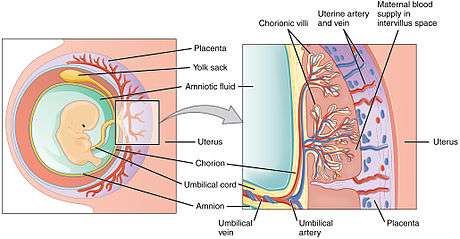 Schematic view of the placenta
Schematic view of the placenta- Maternal side of a whole human placenta, just after birth
 Fetal side of same placenta
Fetal side of same placenta Ziheche (紫河车), dried human placenta used in traditional Chinese medicine
Ziheche (紫河车), dried human placenta used in traditional Chinese medicine
See also
References
- ↑ Pough et al. 1992. Herpetology: Third Edition. Pearson Prentice Hall:Pearson Education, Inc., 2002.
- ↑ Henry George Liddell, Robert Scott, "A Greek-English Lexicon", at Perseus.
- ↑ "placenta". Online Etymology Dictionary.
- ↑ Definitions of placental- related terms.
- ↑ Examination of the placenta
- ↑ Placental Structure and Classification
- 1 2 3 Fox, Chelsea; Eichelberger, Kacey (2015). "Maternal microbiome and pregnancy outcomes". Fertility and Sterility. 104 (6): 1358–1363. doi:10.1016/j.fertnstert.2015.09.037. ISSN 0015-0282. PMID 26493119.
- 1 2 3 Wassenaar, T.M.; Panigrahi, P. (2014). "Is a foetus developing in a sterile environment?". Letters in Applied Microbiology. 59 (6): 572–579. doi:10.1111/lam.12334. ISSN 0266-8254. PMID 25273890.
- ↑ Placental blood circulation
- 1 2 Kiserud T, Acharya G (2004). "The fetal circulation". Prenatal Diagnosis. 24 (13): 1049–1059. doi:10.1002/pd.1062. PMID 15614842.
- 1 2 Reiter, R. J.; Tan, D. X.; Korkmaz, A.; Rosales-Corral, S. A. (2013). "Melatonin and stable circadian rhythms optimize maternal, placental and fetal physiology". Human Reproduction Update. 20 (2): 293–307. doi:10.1093/humupd/dmt054. ISSN 1355-4786. PMID 24132226.
- ↑ Prendiville WJ, Elbourne D, McDonald S (2000). "Active versus expectant management in the third stage of labour". The Cochrane Database of Systematic Reviews (3): CD000007. doi:10.1002/14651858.CD000007. PMID 10908457.
- ↑ Mercer JS, Vohr BR, Erickson-Owens DA, Padbury JF, Oh W (2010). "Seven-month developmental outcomes of very low birth weight infants enrolled in a randomized controlled trial of delayed versus immediate cord clamping". Journal of Perinatology. 30 (1): 11–6. doi:10.1038/jp.2009.170. PMC 2799542
 . PMID 19847185.
. PMID 19847185. - ↑ Wright, Caroline; Sibley, Colin P. (2011). "Placental Transfer in Health and Disease". In Helen Kay, Michael Nelson, and Yuping Wang. The Placenta: From Development to Disease. John Wiley and Sons. p. 66. ISBN 9781444333664.
- ↑ Kappen, Claudia; Kruger, Claudia. (2012). Carlos Penha-Goncalves, ed. "Maternal Diet Modulates Placenta Growth and Gene Expression in a Mouse Model of Diabetic Pregnancy". doi:10.1371/journal.pone.0038445. PMC 3372526.
- ↑ Simister, N. E., and Story, C. M. 1997. "Human placental Fc receptors and the transmission of antibodies from mother to fetus." Journal of Reproductive Immunology 37: 1-23
- ↑ Page 202 in: Pillitteri, Adele (2009). Maternal and Child Health Nursing: Care of the Childbearing and Childrearing Family. Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 1-58255-999-6.
- ↑ Handwerger S, Freemark M (2000). "The roles of placental growth hormone and placental lactogen in the regulation of human fetal growth and development". Journal of Pediatric Endocrinology & Metabolism. 13 (4): 343–56. doi:10.1515/jpem.2000.13.4.343. PMID 10776988.
- ↑ http://www.ucsfhealth.org/tests/003915.html[]
- ↑ "Placenta 'fools body's defences'". BBC News. 10 November 2007.
- ↑ Clark DA, Chaput A, Tutton D (March 1986). "Active suppression of host-vs-graft reaction in pregnant mice. VII. Spontaneous abortion of allogeneic CBA/J x DBA/2 fetuses in the uterus of CBA/J mice correlates with deficient non-T suppressor cell activity". J. Immunol. 136 (5): 1668–75. PMID 2936806.
- ↑ Williams Z, Zepf D, Longtine J, Anchan R, Broadman B, Missmer SA, Hornstein MD (March 2008). "Foreign fetal cells persist in the maternal circulation". Fertil. Steril. 91 (6): 2593–5. doi:10.1016/j.fertnstert.2008.02.008. PMID 18384774.
- ↑ Assad RS, Lee FY, Hanley FL (2001). "Placental compliance during fetal extracorporeal circulation". Journal of applied physiology (Bethesda, Md. : 1985). 90 (5): 1882–1886. PMID 11299282.
- 1 2 "Why eat a placenta?". BBC. 18 April 2006. Retrieved 8 January 2008.
- ↑ Metge, Joan. 2005. "Working in/Playing with three languages: English, Te Reo Maori, and Maori Bod Language." In Sites N.S vol. 2, No 2:83-90.
- ↑ Francisco, Edna (3 December 2004). "Bridging the Cultural Divide in Medicine". Minority Scientists Network. Retrieved 7 January 2008.
- ↑ Shepardson, Mary (1978). "Changes in Navajo Mortuary Practices and Beliefs". American Indian Quarterly. University of Nebraska Press. JSTOR 0095182x.
- 1 2 Buckley, Sarah J. "Placenta Rituals and Folklore from around the World". Mothering. Archived from the original on 6 January 2008. Retrieved 7 January 2008.
- ↑ Davenport, Ann (June 2005). "The Love Offer". Johns Hopkins Magazine. Retrieved 7 January 2008.
- ↑ Falcao, Ronnie. "Medicinal Uses of the Placenta". Retrieved 25 November 2008.
External links
| Wikimedia Commons has media related to Placenta. |
| Look up placenta in Wiktionary, the free dictionary. |
- Additional Human placenta photography
- The Placenta, gynob.com, with quotes from Williams Obstetrics, 18th Edition, F. Gary Cunningham, M.D., Paul C. MacDonald, M.D., Norman F. Grant, M.D., Appleton & Lange, Publishers.
- Evaluation of Hydropic Placentas, by Miller RT, (PDF), ProPath.