Voriconazole
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation | vor-i-KON-a-zole |
| Trade names | Vfend |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a605022 |
| License data |
|
| Pregnancy category |
|
| Routes of administration | IV, by mouth (tablets, oral suspension) |
| ATC code | J02AC03 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 96% (oral administration) |
| Protein binding | 58% |
| Metabolism | Liver: CYP2C19 (significant involvement), also CYP2C9, CYP3A4 |
| Metabolites | Voriconazole N-oxide (major; minimal antifungal activity) |
| Biological half-life | Dose-dependent |
| Excretion | Urine (80–83%)[1] |
| Identifiers | |
| |
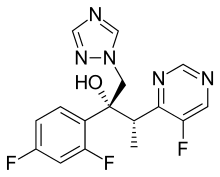
| Synonyms | (αR,βS)-α-(2,4-Difluorophenyl)-5-fluoro-β-methyl-α-(1H-1,2,4-triazol-1-ylmethyl)-4-pyrimidineethanol[2] |
| CAS Number |
137234-62-9 |
| PubChem (CID) | 71616 |
| DrugBank |
DB00582 |
| ChemSpider |
64684 |
| UNII |
JFU09I87TR |
| KEGG |
D00578 |
| ChEBI |
CHEBI:10023 |
| ChEMBL |
CHEMBL638 |
| Chemical and physical data | |
| Formula | C16H14F3N5O |
| Molar mass | 349.311 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| (verify) | |
Voriconazole (INN,[2] brand name Vfend VEE-fend, manufactured by Pfizer) is a triazole antifungal medication that is generally used to treat serious, invasive fungal infections. These are generally seen in patients who are immunocompromised, and include invasive candidiasis, invasive aspergillosis, and certain emerging fungal infections.[3]
Indications
Invasive aspergillosis
Voriconazole is used to treat invasive aspergillosis, which may occur in immunocompromised patients, including allogeneic BMT, hematologic cancers, and solid organ transplants.[3][4]
For multiple site or CNS aspergillosis a combination therapy of voriconazole and liposomal amphotericin B should be considered. It is also the recommended treatment for the CNS fungal infections transmitted by epidural injection of contaminated steroids.[5]
Candidemia
Voriconazole has proven to be as effective as a regimen of intravenous amphotericin B followed by oral fluconazole in patients with culture-proven candidemia. Voriconazole cleared Candida from the bloodstream as quickly as amphotericin B (median 2 days) and showed a trend toward better survival. Voriconazole was also associated with fewer serious adverse events and cases of renal toxicity, but a higher incidence of visual disturbances.[6]
Voriconazole was also proven to offer similar, near-complete efficacy to fluconazole in the treatment of esophageal candidiasis.[7]
Empirical antifungal therapy
A study compared voriconazole use to that of amphotericin B in the treatment of patients with unresolved fever despite broad-spectrum antibiotic therapy who are at risk for breakthrough fungal infections. While overall success rates were 26% for voriconazole and 30.6% for liposomal amphotericin B, there were significantly fewer breakthrough infections with voriconazole, particularly in the patients at highest risk. This study found similar fewer severe reactions and nephrotoxicity but more transient visual disturbances and hallucinations. Voriconazole was also associated with a shorter duration of hospitalization. The authors of this study concluded, "This study demonstrates that voriconazole, a second-generation triazole, is an appropriate agent for empirical antifungal therapy and that its use may reduce the frequency of proven breakthrough fungal infections, preserve renal function, and reduce the frequency of acute infusion-related toxic effects. Formulations of amphotericin B have been the standard of empirical antifungal therapy for nearly 20 years. As this study shows, a second-generation triazole can be used in lieu of amphotericin B for early antifungal therapy."[8]
Efficacy against emerging fungal pathogens
In collected case studies, voriconazole has also been proven effective against a number of other serious fungal pathogens. This includes infections by Fusarium spp. and Scedosporium apiospermum (asexual form of Pseudallescheria boydii). Although infrequently seen, these molds are emerging as more common and deadly causes of fungal infection in seriously immunocompromised patients, and the development of voriconazole has been an important advance in their treatment as they are generally resistant to other antifungal agents (including amphotericin B). Voriconazole is the first and only drug ever specifically indicated for their treatment by the FDA.
Voriconazole has also been used to treat severe fungal corneal infections.
Pharmacokinetics
Voriconazole is well absorbed orally with a bioavailability of 96%, allowing patients to be switched between intravenous and oral administration.
Being metabolized by hepatic cytochrome P450, voriconazole interacts with some drugs. Administration is contraindicated with some drugs (such as sirolimus, rifampicin, rifabutin, carbamazepine, quinidine and ergot alkaloids) and dose adjustments and/or monitoring when coadministered with others (including fluconazole, warfarin, ciclosporin, tacrolimus, omeprazole, and phenytoin). Voriconazole may be safely administered with cimetidine, ranitidine, indinavir, macrolide antibiotics, mycophenolate, digoxin and prednisolone.[1]
Because voriconazole is metabolized by the liver, the dose should be halved in patients with mild-to-moderate hepatic impairment (Child-Pugh score A or B). There are no data available for patients with severe hepatic impairment (Child-Pugh C).
No dose adjustment is necessary for renal impairment or advanced age, but children seem to clear voriconazole faster than adults and drug levels may need monitoring.[9]

Side effects
The most common side effects associated with voriconazole include transient visual disturbances, fever, rash, vomiting, nausea, diarrhea, headache, sepsis, peripheral edema, abdominal pain, and respiratory disorder.
Unlike most adverse effects, which are similar to other azole antifungal agents, visual disturbances (such as blurred vision, color vision change or increased sensitivity to light) are unique to voriconazole. These have been reported by more than 30% of patients in clinical trials. They generally occur approximately one-half hour after administration, and last approximately 30 minutes. In some patients they may go away after continued use. Studies have shown that there is no damage to the eye or long-term effect on vision. However, patients taking voriconazole should be advised against driving at night or other potentially hazardous tasks.
Though rare, there have been cases of serious hepatic reactions during treatment with voriconazole (a class effect of azole antifungal agents). Liver function tests should be evaluated at the start of and during the course of therapy.
Voriconazole is phototoxic. It has been associated with an increased risk of squamous cell carcinoma of the skin.[10]
References
- 1 2 "Vfend (voriconazole) Tablets for Oral Use, for Oral Suspension, for Injection for Intravenous Use. Full Prescribing Information". Roerig, Division of Pfizer, Inc., NY, NY 10017. Retrieved 6 November 2016.
- 1 2 "International Nonproprietary Names for Pharmaceutical Substances (INN). Recommended International Nonproprietary Names (Rec. INN): List 36" (PDF). WHO Drug Information. World Health Organization. 10 (3): 162. 1996. Retrieved 6 November 2016.
- 1 2 Walsh, TJ; Anaissie, EJ; Denning, DW; Herbrecht, R; Kontoyiannis, DP; Marr, KA; Morrison, VA; Segal, BH; Steinbach, WJ; Stevens, DA; van Burik, JA; Wingard, JR; Patterson, TF (1 February 2008). "Treatment of Aspergillosis: Clinical Practice Guidelines of the Infectious Diseases Society of America" (PDF). Clinical Infectious Diseases. 46 (3): 327–60. doi:10.1086/525258. PMID 18177225. Retrieved 6 November 2016.
- ↑ Herbrecht, R; Denning, DW; Patterson, TF; Bennett, JE; Greene, RE; Oestmann, JW; Kern, WV; Marr, KA; Ribaud, P; Lortholary, O; Sylvester, R; Rubin, RH; Wingard, JR; Stark, P; Durand, C; Caillot, D; Thiel, E; Chandrasekar, PH; Hodges, MR; Schlamm, HT; Troke, PF; de Pauw, B (8 August 2002). "Voriconazole versus Amphotericin B for Primary Therapy of Invasive Aspergillosis". The New England Journal of Medicine. 347 (6): 408–15. doi:10.1056/NEJMoa020191. PMID 12167683. Retrieved 6 November 2016.
- ↑ "Multistate Outbreak of Fungal Meningitis and Other Infections — Resources for Clinicians. Interim Treatment Guidance for Central Nervous System and Parameningeal Infections Associated with Injection of Contaminated Steroid Products". Centers for Disease Control and Prevention. Retrieved 6 November 2016.
- ↑ Kullberg, BJ; Sobel, JD; Ruhnke, M; Pappas, PG; Viscoli, C; Rex, JH; Cleary, JD; Rubinstein, E; Church, LWP; Brown, JM; Schlamm, HT; Oborska, IT; Hilton, F; Hodges, MR (22 October 2015). "Voriconazole Versus a Regimen of Amphotericin B Followed by Fluconazole for Candidaemia in Non-neutropenic Patients: a Randomised Non-inferiority Trial". Lancet. 366 (9495): 1435–42. doi:10.1016/S0140-6736(05)67490-9. PMID 16243088.
- ↑ Ally, R; Schürmann, D; Kreisel, W; Carosi, G; Aguirrebengoa, K; Dupont, B; Hodges, M; Troke, P; Romero, AJ (1 November 2001). "A Randomized, Double-Blind, Double-Dummy, Multicenter Trial of Voriconazole and Fluconazole in the Treatment of Esophageal Candidiasis in Immunocompromised Patients" (PDF). Clinical Infectious Diseases. 33 (9): 1447–54. doi:10.1086/322653. PMID 11577374. Retrieved 6 November 2016.
- ↑ Walsh, TJ; Pappas, P; Winston, DJ; Lazarus, HM; Petersen, F; Raffali, J; Yanovich, S; Stiff, P; Greenberg, R; Donowitz, G; Schuster, M; Reboli, A; Wingard, J; Arndt, C; Reinhard, J; Hadley, S; Finberg, R; Laverdière, M; Perfect, J; Garber, G; Fioritoni, G; Anaissie, E; Lee, J (24 January 2002). "Voriconazole Compared with Liposomal Amphotericin B for Empirical Antifungal Therapy in Patients with Neutropenia and Persistent Fever". The New England Journal of Medicine. 346 (4): 225–34. doi:10.1056/NEJM200201243460403. PMID 11807146. Retrieved 6 November 2016.
- ↑ Smith, J; Safdar, N; Knasinski, V; Simmons, W; Bhavnani, SM; Ambrose, PG; Andes, D (April 2006). "Voriconazole Therapeutic Drug Monitoring" (PDF). Antimicrobial Agents and Chemotherapy. 50 (4): 1570–2. doi:10.1128/AAC.50.4.1570-1572.2006. PMC 1426935
 . PMID 16569888. Retrieved 6 November 2016.
. PMID 16569888. Retrieved 6 November 2016. - ↑ Epaulard, O; Saint-Raymond, C; Villier, C; Charles, J; Roch, N; Beani, JC; Leccia, MT (September 2010). "Multiple Aggressive Squamous Cell Carcinomas Associated with Prolonged Voriconazole Therapy in Four Immunocompromised Patients". Clinical Microbiology and Infection. 16 (9): 1362–4. doi:10.1111/j.1469-0691.2009.03124.x. PMID 19930272. Retrieved 6 November 2016.