Drug eruption
| Drug eruption | |
|---|---|
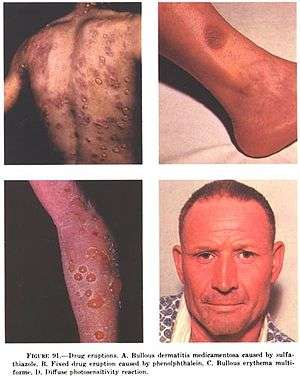 | |
| Examples of drug eruptions. (A) Bullous dermatitis caused by sulfathiazole (B) Fixed drug eruption caused by phenolphtalein (C) Bullous erythema multiforme (D) Diffuse photosensitivity reaction. | |
| Classification and external resources | |
| Specialty | dermatology |
| ICD-10 | L27.0, L27.1 |
| ICD-9-CM | 692.3, 782.1 |
| eMedicine | derm/104 |
| MeSH | D003875 |
In medicine, a drug eruption is an adverse drug reaction of the skin. Most drug-induced cutaneous reactions are mild and disappear when the offending drug is withdrawn.[1] These are called "simple" drug eruptions. However, more serious drug eruptions may be associated with organ injury such as liver or kidney damage and are categorized as "complex".[2] Drugs can also cause hair and nail changes, affect the mucous membranes, or cause itching without outward skin changes.[3]
Diagnosis
Drug eruptions are diagnosed mainly from the medical history and clinical examination. However, they can mimic a wide range of other conditions, thus delaying diagnosis (for example, in drug-induced lupus erythematosus, or the acne-like rash caused by erlotinib). A skin biopsy, blood tests or immunological tests can also be useful. If the causative agent cannot be withdrawn, the symptoms should be relieved as much as possible.
It is estimated that 2—3 percent of hospitalised patients are affected by a drug eruption, and that serious drug eruptions occur in around 1 in 1000 patients.[4]
Drug reactions have characteristic timing. The typical amount of time it takes for a rash to appear after exposure to a drug can help categorize the type of reaction. For example, Acute generalized exanthematous pustulosis usually occurs within 4 days of starting the culprit drug. Drug Reaction with Eosinophilia and Systemic Symptoms usually occurs between 15 and 40 days after exposure. Toxic epidermal necrolysis and Stevens-Johnson syndrome typically occur 7–21 days after exposure. Anaphylaxis occurs within minutes. Simple exanthematous eruptions occur between 4 and 14 days after exposure.[2]
Classification
The drug eruption can be an expected adverse effect or an unexpected effect (idiosyncratic).
Some of the most severe and life-threatening examples of drug eruptions are erythema multiforme, Stevens–Johnson syndrome, toxic epidermal necrolysis, hypersensitivity vasculitis, DRESS syndrome, erythroderma and exanthematous pustulosis.
By appearance
The most common type of eruption is a morbilliform (resembling measles) or erythematous rash, but the appearance may also be urticarial, papulosquamous, pustular, purpuric, bullous (with blisters) or lichenoid.[3] Angioedema can also be drug-induced (most notably, by angiotensin converting enzyme inhibitors).
By mechanism
The underlying mechanism can be immunological (such as in drug allergies) or non-immunological (for example, in photodermatitis or as a side effect of anticoagulants). A fixed drug eruption is the term for a drug eruption that occurs in the same skin area every time the person is exposed to the drug. Eruptions can occur frequently with a certain drug (for example, with phenytoin[5]), or be very rare (for example, Sweet's syndrome following the administration of colony-stimulating factors[6]).
By drug
The culprit can be both a prescription drug or an over-the-counter medication.
Examples of common drugs causing drug eruptions are antibiotics and other antimicrobial drugs, sulfa drugs, nonsteroidal anti-inflammatory drugs (NSAIDs), biopharmaceuticals, chemotherapy agents, anticonvulsants, and psychotropic drugs. Common examples include photodermatitis due to local NSAIDs (such as piroxicam) or due to antibiotics (such as minocycline), and the rash following ampicillin in cases of mononucleosis.
Certain drugs are less likely to cause drug eruptions (rates estimated to be ≤3 per 1000 patients exposed). These include: digoxin, aluminum hydroxide, multivitamins, acetaminophen, bisacodyl, aspirin, thiamine, prednisone, atropine, codeine, hydrochlorothiazide, morphine, insulin, warfarin, and spironolactone.[2] This does not count phototoxic reactions.
References
- ↑ Manders SM (June 1995). "Serious and life-threatening drug eruptions". Am Fam Physician. 51 (8): 1865–72. PMID 7762478.
- 1 2 3 Schaffer (2012). Jean L. Bolognia; Joseph L. Jorizzo; Julie V., eds. Dermatology (3rd ed.). [Philadelphia]: Elsevier Saunders. ISBN 978-0723435716.
- 1 2 Valeyrie-Allanore L, Sassolas B, Roujeau JC (2007). "Drug-induced skin, nail and hair disorders". Drug Saf. 30 (11): 1011–30. doi:10.2165/00002018-200730110-00003. PMID 17973540.
- ↑ Roujeau JC, Stern RS (November 1994). "Severe adverse cutaneous reactions to drugs". N. Engl. J. Med. 331 (19): 1272–85. doi:10.1056/NEJM199411103311906. PMID 7794310.
- ↑ Scheinfeld N (August 2003). "Phenytoin in cutaneous medicine: its uses, mechanisms and side effects". Dermatol. Online J. 9 (3): 6. PMID 12952753.
- ↑ Cohen PR (2007). "Sweet's syndrome--a comprehensive review of an acute febrile neutrophilic dermatosis". Orphanet J Rare Dis. 2: 34. doi:10.1186/1750-1172-2-34. PMC 1963326
 . PMID 17655751.
. PMID 17655751.