Cluster headache
| Cluster headache | |
|---|---|
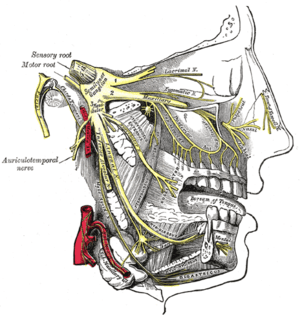 | |
| Trigeminal nerve | |
| Classification and external resources | |
| Specialty | Neurology |
| ICD-10 | G44.0 |
| ICD-9-CM | 339.00,339.01,339.02, |
| DiseasesDB | 2850 |
| MedlinePlus | 000786 |
| eMedicine | EMERG/229 article/1142459 |
| Patient UK | Cluster headache |
| MeSH | D003027 |
Cluster headache (CH) is a neurological disorder characterized by recurrent, severe headaches on one side of the head, typically around the eye.[1] There are often accompanying autonomic symptoms during the headache such as eye watering, nasal congestion and swelling around the eye, typically confined to the side of the head with the pain.[1]
Cluster headache belongs to a group of primary headache disorders, classified as the trigeminal autonomic cephalalgias or (TACs). Cluster headache is named after the demonstrated grouping of headache attacks occurring together (cluster).[1] Individuals typically experience repeated attacks of excruciatingly severe unilateral headache pain.[2] Cluster headache attacks often occur periodically; spontaneous remissions may interrupt active periods of pain, though about 10–15% of chronic CH never remit.[2] The cause of cluster headache has not been identified.
While there is no known cure, cluster headaches can sometimes be prevented and acute attacks treated. Recommended treatments for acute attacks include oxygen or a fast acting triptan.[3] Primary recommended prevention is verapamil. Steroids may be used as a transitional treatment and may prevent attack recurrence until preventative treatments take effect. The condition affects approximately 0.2% of the general population,[4] and men are more commonly affected than women, by a ratio of about 2.5:1 to 3.5:1.[1]
Signs and symptoms
Cluster headaches are recurring bouts of excruciating unilateral headache attacks[5] of extreme intensity.[6] The duration of a typical CH attack ranges from about 15 to 180 minutes.[3] Most untreated attacks (about 75%) last less than 60 minutes.[7]
The onset of an attack is rapid and most often without preliminary signs that are characteristic in migraine. Preliminary sensations of pain in the general area of attack, referred to as "shadows", may signal an imminent CH, or these symptoms may linger after an attack has passed, or even between attacks.[8] Though CH is strictly unilateral, there are some documented cases of "side-shift" between cluster periods, extremely rare, simultaneously (within the same cluster period) bilateral headache.[9]
Pain
The pain occurs only on one side of the head (unilateral), around the eye (orbital), particularly above the eye (supraorbital), in the temple (temporal), or in any combination. The pain of CH attack is remarkably greater than in other headache conditions, including severe migraine. The pain is typically described as burning, stabbing, boring or squeezing, and may be located near or behind the eye.[10] Those with cluster headaches may experience suicidal thoughts during an attack as a result of the pain.[11][12] It is reported as one of the most painful conditions.[13]
Other symptoms
The typical symptoms of cluster headache include grouped occurrence and recurrence (cluster) of headache attack, severe unilateral orbital, supraorbital and/or temporal pain. If left untreated, attack frequency may range from one attack every two days to eight attacks per day.[2][3] Cluster headache attack is accompanied by at least one of the following autonomic symptoms: drooping eyelid, pupil constriction, redness of the conjunctiva, tearing, runny nose, and less commonly, facial blushing, swelling, or sweating, typically appearing on the same side of the head as the pain.[2]
Restlessness (for example, pacing or rocking back and forth), photosensitivity, aversion to light (photophobia) or sensitivity to noise (phonophobia) may occur during a CH. Nausea is a rare symptom, although it has been reported.[5] Secondary effects may include inability to organize thoughts and plans, physical exhaustion, confusion, agitation, aggressiveness, depression and anxiety.[14]
People with CH may dread facing another headache and adjust their physical or social activities around a possible future occurrence. Likewise they may seek assistance to accomplish what would otherwise be normal tasks. They may hesitate to make plans because of the regularity, or conversely, the unpredictability of the pain schedule. These factors can lead to generalized anxiety disorders, panic disorder,[15] serious depressive disorders,[16] social withdrawal and isolation.[17]
Recurrence
Cluster headaches may occasionally be referred to as "alarm clock headache" because of the regularity of their recurrence. CH attacks may awaken individuals from sleep. Both individual attacks and the cluster grouping can have a metronomic regularity; attacks typically striking at a precise time of day each morning or night. The recurrence of headache cluster grouping may occur more often around solstices, or spring and autumn equinoxes, sometimes showing circannual periodicity. Conversely, attack frequency may be highly unpredictable, showing no periodicity at all. These observations have prompted researchers to speculate an involvement, or dysfunction of the hypothalamus. The Hypothalamus controls the body's "biological clock" and circadian rhythm.[18][19] In episodic cluster headache, attacks occur once or more daily, often at the same time each day for a period of several weeks, followed by a headache-free period lasting weeks, months, or years. Approximately 10–15% of cluster headaches are chronic, with multiple headaches occurring every day for years, sometimes without any remission.
In accordance with the International Headache Society (IHS) diagnostic criteria, cluster headaches occurring in two or more cluster periods, lasting from 7 to 365 days with a pain-free remission of one month or longer between the headache attacks, may be classified as episodic. If headache attacks occur for more than a year without pain-free remission of at least one month, the condition is classified as chronic.[2] Chronic CH both occurs and recurs without any remission periods between cycles; there may be variation in cycles, meaning the frequency and severity of attacks may change without predictability for a period of time. The frequency, severity and duration of headache attacks experienced by people during these cycles varies between individuals and does not demonstrate complete remission of the episodic form. The condition may change unpredictably, from chronic to episodic and from episodic to chronic.[20]
Causes
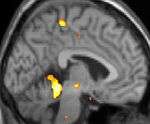 |  |  |
| Positron emission tomography (PET) shows brain areas being activated during pain | ||
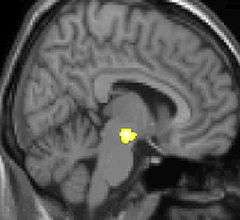 | 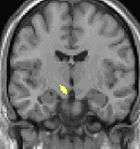 | 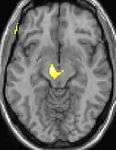 |
| Voxel-based morphometry (VBM) shows brain area structural differences | ||
The cause of cluster headache is unknown.[21]
Genetics
Cluster headache may, but rarely, run in some families in an autosomal dominant inheritance pattern.[21] People with a first degree relative with the condition are about 14-48 times more likely to develop it themselves,[1] and between 1.9 and 20% of persons with CH have a positive family history.[21] Possible genetic factors warrant further research, current evidence for genetic inheritance is limited.[21]
Tobacco smoking
About 65% of persons with CH are, or have been, tobacco smokers.[1] Stopping smoking does not lead to improvement of the condition and CH also occurs in those who have never smoked (e.g. children);[1] it is thought unlikely that smoking is a cause.[1] People with CH may be predisposed to certain traits, including smoking or other lifestyle habits.[22]
Hypothalamus
Some theories suggest that CH attacks may be related to dysfunction of the hypothalamus, this may explain why cluster headaches frequently occur around the same time each day, and during a particular season. One of the functions of the hypothalamus is regulation of the biological clock. Metabolic abnormalities have also been reported. Positron emission tomography (PET) scans indicate the brain areas which are activated during attack only, compared to pain free periods. These pictures show brain areas which are active during pain in yellow/orange color (called "pain matrix"). The area in the center (in all three views) is specifically activated during CH only. The bottom row voxel-based morphometry (VBM) shows structural brain differences between individuals with and without CH; only a portion of the hypothalamus is different.[23]
Pathophysiology
Cluster headache has been historically described as vascular headaches; for decades, it has been proposed that intense pain was caused by dilation of blood vessels which in turn, was thought to create pressure on the trigeminal nerve. While this theory was thought to be the immediate cause of the pain, the etiology (underlying cause or causes) is not fully understood. CH pathogenesis is the subject of ongoing debate.[24] Investigations into vascular theories of headache disorders are helping to identify the role of other possible causative mechanisms in CH.[25]
Diagnosis
Cluster headaches are often misdiagnosed, mismanaged, or undiagnosed for many years; they may be confused with migraine, "cluster-like" headache (or mimics), CH subtypes, other TACs ( trigeminal autonomic cephalalgias), or other types of primary or secondary headache syndrome.[26] Cluster-like head pain may be diagnosed as secondary headache rather than cluster headache.[2]
A detailed oral history aids practitioners in correct differential diagnosis, as there are no confirmatory tests for CH. A headache diary can be useful in tracking when and where pain occurs, how severe it is, and how long the pain lasts. A record of coping strategies used may help distinguish between headache type; data on frequency, severity and duration of headache attacks are a necessary tool for initial and correct differential diagnosis in headache conditions.[27]
Correct diagnosis of CH presents a challenge as the first attack may present where staff are not trained in the diagnosis of rare or complex chronic disease.[28] Although experienced ER staff are sometimes trained to detect headache types,[29] CH attacks themselves are not life-threatening.[30]
Individuals with CH typically experience diagnostic delay before correct diagnosis.[26][31] People are often misdiagnosed due to reported neck, tooth, jaw, and sinus symptoms and may unnecessarily endure many years of referral to ear, nose and throat (ENT) specialists for investigation of sinuses; dentists for tooth assessment; chiropractors and manipulative therapists for treatment; or psychiatrists, psychologists and other medical disciplines before their headaches are correctly diagnosed.[32] Under-recognition of CH by health care professionals is reflected in consistent findings in Europe and the United States that the average time to diagnosis is around seven years.[33] Medical students receive little training in differential diagnoses and management of headaches.[34]
Differential
Cluster headache may be misdiagnosed as migraine or sinusitis.[33] Other types of headache are sometimes mistaken for, or may mimic closely, CH. Incorrect terms like "cluster migraine" confuse headache types, confound differential diagnosis and are often the cause of unnecessary diagnostic delay,[35] ultimately delaying appropriate specialist treatment.
Headaches that may be confused with CH include:
- Chronic paroxysmal hemicrania (CPH) is a unilateral headache condition, without the male predominance usually seen in CH. Paroxysmal hemicrania may also be episodic. CPH typically responds "absolutely" to treatment with the anti-inflammatory drug indomethacin[2] where in most cases CH typically shows no positive indomethacin response, making "Indomethacin response" an important diagnostic tool for specialist practitioners seeking correct differential diagnosis between the conditions.
- Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) is a headache syndrome belonging to the group of TACs.[2][36]
- Trigeminal neuralgia is a unilateral headache syndrome,[32] or "cluster-like" headache.[37]
Prevention
Preventive treatments are used to reduce or eliminate cluster headache attacks; they are generally used in combination with abortive and transitional techniques.[5]
Verapamil
The recommended first-line preventative therapy is verapamil, a calcium channel blocker.[3][38] Verapamil was previously underused in people with cluster headache.[5]
Steroids
There is little evidence to support a long-term benefit from steroids,[3] but they may be used until other medications take effect as they appear to be effective at three days.[3] They are generally discontinued after 8–10 days of treatment.[5]
Surgery
Nerve stimulators may be an option in the small number of people who do not improve with medications.[39][40] Two procedures, deep brain stimulation or occipital nerve stimulation, may be useful;[3] early experience shows a benefit in about 60% of cases.[41] It typically takes weeks or months for this benefit to appear.[40] A non-invasive method using transcutaneous electrical nerve stimulation (TENS) is being studied.[40]
A number of surgical procedures, such as a rhizotomy or microvascular decompression, may also be considered,[40] but evidence to support them is limited and there are cases of people ending up worse off.[40]
Other
Lithium, methysergide, and topiramate are recommended alternative treatments,[38][42] although there is little evidence supporting the use of topiramate or methysergide.[3][43] This is also true for tianeptine, melatonin and ergotamine.[3] Valproate, sumatriptan and oxygen are not recommended as preventative measures.[3] Botulinum toxin injections have shown limited success.[44] Evidence for baclofen, botulinum toxin, and capsaicin is unclear.[43]
Management
Treatment for cluster headache is divided into three primary categories: abortive, transitional, and preventative.[45] There are two primary treatments for acute CH: oxygen and triptans,[3] but they are underused due to misdiagnosis of the syndrome.[5] During bouts of headaches, triggers such as alcohol, nitroglycerine and naps during the day should be avoided.[7]
Oxygen
Oxygen therapy may help people with CH, but it does not help prevent future episodes.[3] Typically it is given via a non-rebreather mask at 12-15 liters per minute for 15–20 minutes.[3] Around 70% improve within 15 minutes.[7]
Triptans
The other primarily recommended treatment of acute attacks is subcutaneous or intranasal sumatriptan.[38] Sumatriptan and zolmitriptan have both been shown to improve symptoms during an attack with sumatriptan being superior.[46] Because of the vasoconstrictive side-effect of triptans, they may be contraindicated in people with ischemic heart disease.[3]
Opioids
The use of opioid medication in management of CH is not recommended[47] and may make headache syndromes worse.[48][49] Long-term opioid use is associated with well known dependency, addiction and withdrawal syndromes.[50] Prescription of opioid medication may additionally lead to further delay in differential diagnosis, undertreatment, and mismanagement.[47]
Other
The vasoconstrictor ergot compounds may be useful,[7] but have not been well studied in acute attacks.[46] Octreotide administered subcutaneously has been demonstrated to be more effective than placebo for the treatment of acute attacks.[51]
Epidemiology
Cluster headache affects about 0.2% of the general population,[4] or 56 to 326 people per 100,000.[52] Males are affected more commonly than females, in a ratio of about 2.5:1 to 3.5:1.[1] The condition usually starts between the ages of 20 and 50 years, although it can occur at any age.[1]
History
The first complete description of cluster headache was given by the London neurologist Wilfred Harris in 1926, who named the disease migrainous neuralgia.[53][54][55] Descriptions of CH date to 1745 and probably earlier.[56]
The condition was originally named Horton's cephalalgia after Bayard Taylor Horton, a US neurologist who postulated the first theory as to their pathogenesis. His original paper describes the severity of the headaches as being able to take normal men and force them to attempt or complete suicide; his 1939 paper said:
"Our patients were disabled by the disorder and suffered from bouts of pain from two to twenty times a week. They had found no relief from the usual methods of treatment. Their pain was so severe that several of them had to be constantly watched for fear of suicide. Most of them were willing to submit to any operation which might bring relief."[57]
CH has alternately been called erythroprosopalgia of Bing, ciliary neuralgia, erythromelalgia of the head, Horton's headache, histaminic cephalalgia, petrosal neuralgia, sphenopalatine neuralgia, vidian neuralgia, Sluder's neuralgia, Sluder's syndrome, and hemicrania angioparalyticia.[58]
Society and culture
Robert Shapiro, a professor of neurology, says that while cluster headaches are about as common as multiple sclerosis with a similar disability level, as of 2013, the US National Institutes of Health had spent $1.872 billion on research into multiple sclerosis in one decade, but less than $2 million on CH research in 25 years.[59] Due to an occasional association with suicidal thoughts, cluster headaches have been colloquially named "suicide headaches."[11] There are no approved medicines for the prevention of cluster headache in the United States.[60]
Research directions
Some controversial case reports suggest that ingesting tryptamines such as LSD, psilocybin, or DMT can reduce pain and interrupt cluster headache cycles.[61][62] A 2006 interview/survey of 53 individuals with CH said that psilocybin extended remission periods in 10% cases.[62] The survey was not a blinded or controlled study, and was "limited by recall and selection bias".[61]
References
- 1 2 3 4 5 6 7 8 9 10 Nesbitt AD, Goadsby PJ (Apr 11, 2012). "Cluster headache". BMJ (Clinical research ed.) (Review). 344: e2407. doi:10.1136/bmj.e2407. PMID 22496300.
- 1 2 3 4 5 6 7 8 "IHS Classification ICHD-II 3.1 Cluster headache". The International Headache Society. Retrieved 2014-01-03.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Weaver-Agostoni J (Jul 15, 2013). "Cluster headache". American family physician (Review). 88 (2): 122–8. PMID 23939643.
- 1 2 Bennett MH, French C, Schnabel A, Wasiak J, Kranke P (2008). "Normobaric and hyperbaric oxygen therapy for migraine and cluster headache". Cochrane Database Syst Rev (Review) (3): CD005219. doi:10.1002/14651858.CD005219.pub2. PMID 18646121.
- 1 2 3 4 5 6 Beck E, Sieber WJ, Trejo R (February 2005). "Management of cluster headache". Am Fam Physician (Review). 71 (4): 717–24. PMID 15742909.
- ↑ Capobianco DJ, Dodick DW (April 2006). "Diagnosis and treatment of cluster headache". Semin Neurol (Review). 26 (2): 242–59. doi:10.1055/s-2006-939925. PMID 16628535.
- 1 2 3 4 Friedman BW, Grosberg BM (Feb 2009). "Diagnosis and management of the primary headache disorders in the emergency department setting". Emergency medicine clinics of North America (Review). 27 (1): 71–87, viii. doi:10.1016/j.emc.2008.09.005. PMC 2676687
 . PMID 19218020.
. PMID 19218020. - ↑ Marmura MJ, Pello SJ, Young WB (December 2010). "Interictal pain in cluster headache". Cephalalgia. 30 (12): 1531–4. doi:10.1177/0333102410372423. PMID 20974600.
- ↑ Meyer EL, Laurell K, Artto V, et al. (August 2009). "Lateralization in cluster headache: a Nordic multicenter study". J Headache Pain. 10 (4): 259–63. doi:10.1007/s10194-009-0129-z. PMC 3451747. PMID 19495933.
- ↑ Noshir Mehta; George E. Maloney; Dhirendra S. Bana; Steven J. Scrivani (20 September 2011). Head, Face, and Neck Pain Science, Evaluation, and Management: An Interdisciplinary Approach. John Wiley & Sons. pp. 199–. ISBN 978-1-118-20995-0.
- 1 2 Robbins, MS (Feb 2013). "The psychiatric comorbidities of cluster headache.". Current pain and headache reports. 17 (2): 313. doi:10.1007/s11916-012-0313-8. PMID 23296640.
- ↑ The 5-Minute Sports Medicine Consult (2 ed.). Lippincott Williams & Wilkins. 2012. p. 87. ISBN 9781451148121.
- ↑ Matharu, MS; Goadsby, PJ (September 2004). "Cluster headache: focus on emerging therapies.". Expert Review of Neurotherapeutics. 4 (5): 895–907. doi:10.1586/14737175.4.5.895. PMID 15853515.
- ↑ Robbins MS (Feb 2013). "The psychiatric comorbidities of cluster headache". Current pain and headache reports (REview). 17 (2): 313. doi:10.1007/s11916-012-0313-8. PMID 23296640.
- ↑ Robbins MS (February 2013). "The psychiatric comorbidities of cluster headache". Curr Pain Headache Rep (Review). 17 (2): 313. doi:10.1007/s11916-012-0313-8. PMID 23296640.
- ↑ Liang JF, Chen YT, Fuh JL, et al. (February 2013). "Cluster headache is associated with an increased risk of depression: a nationwide population-based cohort study". Cephalalgia. 33 (3): 182–9. doi:10.1177/0333102412469738. PMID 23212294.
- ↑ Jensen RM, Lyngberg A, Jensen RH (June 2007). "Burden of cluster headache". Cephalalgia. 27 (6): 535–41. doi:10.1111/j.1468-2982.2007.01330.x. PMID 17459083.
- ↑ Pringsheim T (February 2002). "Cluster headache: evidence for a disorder of circadian rhythm and hypothalamic function". Can J Neurol Sci (Review). 29 (1): 33–40. PMID 11858532.
- ↑ Dodick DW, Eross EJ, Parish JM, Silber M (March 2003). "Clinical, anatomical, and physiologic relationship between sleep and headache". Headache. 43 (3): 282–92. doi:10.1046/j.1526-4610.2003.03055.x. PMID 12603650.
- ↑ Torelli P, Manzoni GC (February 2002). "What predicts evolution from episodic to chronic cluster headache?". Curr Pain Headache Rep (Review). 6 (1): 65–70. doi:10.1007/s11916-002-0026-5. PMID 11749880.
- 1 2 3 4 Pinessi L, Rainero I, Rivoiro C, Rubino E, Gallone S (September 2005). "Genetics of cluster headache: an update". J Headache Pain (Review). 6 (4): 234–6. doi:10.1007/s10194-005-0194-x. PMC 3452030. PMID 16362673.
- ↑ Schürks M, Diener HC (April 2008). "Cluster headache and lifestyle habits". Curr Pain Headache Rep (Review). 12 (2): 115–21. doi:10.1007/s11916-008-0022-5. PMID 18474191.
- ↑ DaSilva AF, Goadsby PJ, Borsook D (April 2007). "Cluster headache: a review of neuroimaging findings". Curr Pain Headache Rep (Review). 11 (2): 131–6. doi:10.1007/s11916-007-0010-1. PMID 17367592.
- ↑ Goadsby PJ (January 2009). "The vascular theory of migraine--a great story wrecked by the facts". Brain (Review). 132 (Pt 1): 6–7. doi:10.1093/brain/awn321. PMID 19098031.
- ↑ Leone M, Cecchini AP, Tullo V, Curone M, Di Fiore P, Bussone G (May 2013). "Cluster headache: what has changed since 1999?". Neurol. Sci. (Review). 34 Suppl 1: S71–3. doi:10.1007/s10072-013-1365-1. PMID 23695050.
- 1 2 van Vliet JA, Eekers PJ, Haan J, Ferrari MD (August 2003). "Features involved in the diagnostic delay of cluster headache". J. Neurol. Neurosurg. Psychiatr. 74 (8): 1123–5. doi:10.1136/jnnp.74.8.1123. PMC 1738593. PMID 12876249. Lay summary – World Headache Alliance (2003-08-21).
- ↑ "Headache diary: helping you manage your headache" (PDF). NPS.org.au. Retrieved 2014-01-02.
- ↑ Friedman BW, Grosberg BM (February 2009). "Diagnosis and management of the primary headache disorders in the emergency department setting". Emerg. Med. Clin. North Am. (Review). 27 (1): 71–87, viii. doi:10.1016/j.emc.2008.09.005. PMC 2676687. PMID 19218020.
- ↑ Clarke CE, Edwards J, Nicholl DJ, Sivaguru A, Davies P, Wiskin C (August 2005). "Ability of a nurse specialist to diagnose simple headache disorders compared with consultant neurologists". J. Neurol. Neurosurg. Psychiatr. 76 (8): 1170–2. doi:10.1136/jnnp.2004.057968. PMC 1739753. PMID 16024902.
- ↑ "Cluster headache". MedlinePlus Medical Encyclopedia. 2012-11-02. Retrieved 2014-04-05.
- ↑ Bahra A, Goadsby PJ (March 2004). "Diagnostic delays and mis-management in cluster headache". Acta Neurol. Scand. 109 (3): 175–9. doi:10.1046/j.1600-0404.2003.00237.x. PMID 14763953.
- 1 2 Van Alboom E, Louis P, Van Zandijcke M, Crevits L, Vakaet A, Paemeleire K (March 2009). "Diagnostic and therapeutic trajectory of cluster headache patients in Flanders". Acta Neurol Belg. 109 (1): 10–7. PMID 19402567.
- 1 2 Tfelt-Hansen PC, Jensen RH (Jul 1, 2012). "Management of cluster headache". CNS Drugs (Review). 26 (7): 571–80. doi:10.2165/11632850-000000000-00000. PMID 22650381.
- ↑ Ahmed F (2012). "Headache disorders: differentiating and managing the common subtypes". British Journal of Pain. 6 (3): 124–32. doi:10.1177/2049463712459691.
- ↑ Klapper JA, Klapper A, Voss T (October 2000). "The misdiagnosis of cluster headache: a nonclinic, population-based, Internet survey". Headache. 40 (9): 730–5. doi:10.1046/j.1526-4610.2000.00127.x. PMID 11091291.
- ↑ Alore PL, Jay WM, Macken MP (2006). "SUNCT syndrome: Short-lasting Unilateral Neuralgiform headache with Conjunctival injection and Tearing". Semin Ophthalmol. 21 (1): 9–13. doi:10.1080/08820530500509317. PMID 16517438.
- ↑ Benoliel R (August 2012). "Trigeminal autonomic cephalgias" (PDF). British Journal of Pain. 6 (3): 106–23. doi:10.1177/2049463712456355.
- 1 2 3 May A, Leone M, Afra J, et al. (October 2006). "EFNS guidelines on the treatment of cluster headache and other trigeminal-autonomic cephalalgias" (PDF). Eur J Neurol. 13 (10): 1066–77. doi:10.1111/j.1468-1331.2006.01566.x. PMID 16987158. Archived from the original (PDF) on 7 March 2008.
- ↑ Magis D, Schoenen J (2011). "Peripheral nerve stimulation in chronic cluster headache". Progress in neurological surgery (Review). 24: 126–32. doi:10.1159/000323045. PMID 21422783.
- 1 2 3 4 5 Martelletti P, Jensen RH, Antal A, et al. (Oct 21, 2013). "Neuromodulation of chronic headaches: position statement from the European Headache Federation". The journal of headache and pain. 14 (1): 86. doi:10.1186/1129-2377-14-86. PMID 24144382.
- ↑ Bartsch T, Paemeleire K, Goadsby PJ (June 2009). "Neurostimulation approaches to primary headache disorders". Curr. Opin. Neurol (Review). 22 (3): 262–8. doi:10.1097/wco.0b013e32832ae61e. PMID 19434793.
- ↑ Evers S (Sep 2010). "Pharmacotherapy of cluster headache". Expert opinion on pharmacotherapy (Review). 11 (13): 2121–7. doi:10.1517/14656566.2010.496454. PMID 20569084.
- 1 2 Matharu M (Feb 9, 2010). "Cluster headache". Clinical evidence (Review). 2010. PMC 2907610. PMID 21718584.
- ↑ Ailani J, Young WB (Apr 2009). "The role of nerve blocks and botulinum toxin injections in the management of cluster headaches". Current pain and headache reports (Review). 13 (2): 164–7. doi:10.1007/s11916-009-0028-7. PMID 19272284.
- ↑ Nalini Vadivelu; Alan David Kaye; Jack M. Berger. Essentials of palliative care. New York, NY: Springer. p. 335. ISBN 9781461451648.
- 1 2 Law S, Derry S, Moore RA (Jul 17, 2013). "Triptans for acute cluster headache". The Cochrane database of systematic reviews (Review). 7: CD008042. doi:10.1002/14651858.cd008042.pub3. PMID 24353996.
- 1 2 Paemeleire K, Evers S, Goadsby PJ (April 2008). "Medication-overuse headache in patients with cluster headache". Curr Pain Headache Rep. 12 (2): 122–7. doi:10.1007/s11916-008-0023-4. PMID 18474192.
- ↑ Johnson JL, Hutchinson MR, Williams DB, Rolan P (January 2013). "Medication-overuse headache and opioid-induced hyperalgesia: a review of mechanisms, a neuroimmune hypothesis and a novel approach to treatment". Cephalalgia (Review). 33 (1): 52–64. doi:10.1177/0333102412467512. PMID 23144180.
- ↑ Watkins LR, Hutchinson MR, Rice KC, Maier SF (November 2009). "The "toll" of opioid-induced glial activation: improving the clinical efficacy of opioids by targeting glia". Trends Pharmacol. Sci. (Review). 30 (11): 581–91. doi:10.1016/j.tips.2009.08.002. PMC 2783351. PMID 19762094.
- ↑ Saper JR, Da Silva AN (November 2013). "Medication overuse headache: history, features, prevention and management strategies". CNS Drugs. 27 (11): 867–77. doi:10.1007/s40263-013-0081-y. PMID 23925669.
- ↑ Matharu, M (9 February 2010). "Cluster headache.". Clinical evidence. 2010. PMC 2907610. PMID 21718584.
- ↑ Torelli P, Castellini P, Cucurachi L, Devetak M, Lambru G, Manzoni G (2006). "Cluster headache prevalence: methodological considerations. A review of the literature" (PDF). Acta Biomed Ateneo Parmense (Review). 77 (1): 4–9. PMID 16856701.
- ↑ Harris W.: Neuritis and Neuralgia. p. 307-12. Oxford: Oxford University Press 1926.
- ↑ Bickerstaff E (1959). "The periodic migrainous neuralgia of Wilfred Harris". The Lancet. 273 (7082): 1069–71. doi:10.1016/S0140-6736(59)90651-8. PMID 13655672.
- ↑ Boes CJ, Capobianco DJ, Matharu MS, Goadsby PJ (2002). "Wilfred Harris' early description of cluster headache". Cephalalgia. 22 (4): 320–6. doi:10.1046/j.1468-2982.2002.00360.x. PMID 12100097.
- ↑ Pearce JM (November 2007). "Gerardi van Swieten: descriptions of episodic cluster headache". J. Neurol. Neurosurg. Psychiatr. 78 (11): 1248–9. doi:10.1136/jnnp.2007.123091. PMC 2117620. PMID 17940171.
- ↑ Horton BT, MacLean AR, Craig WM (1939). "A new syndrome of vascular headache: results of treatment with histamine: preliminary report". Mayo Clinic Proc. 14: 257.
- ↑ Silberstein SD, Lipton RB, Goadsby PJ (2002). Headache in Clinical Practice (Second ed.). Taylor & Francis.
- ↑ Johnson, Tim (May 16, 2013). "Researcher works to unlock mysteries of migraines". USA Today. Retrieved January 4, 2013.
- ↑ http://www.prnewswire.com/news-releases/lillys-investigational-medicine-for-prevention-of-migraine-met-primary-endpoint-in-a-phase-2b-study-300100695.html
- 1 2 Sun-Edelstein C, Mauskop A (March 2011). "Alternative headache treatments: nutraceuticals, behavioral and physical treatments". Headache (Review). 51 (3): 469–83. doi:10.1111/j.1526-4610.2011.01846.x. PMID 21352222.
Although controversial, the evidence for the use of psychedelic drugs such as DMT, lysergic acid diethylamide (LSD) and psilocybin is worth mentioning for the insight it provides regarding the pathophysiology of migraine and cluster headache. Further research on the effects of these substances may result in a greater understanding of the mechanisms of these headache disorders. ...
- 1 2 Vollenweider FX, Kometer M (September 2010). "The neurobiology of psychedelic drugs: implications for the treatment of mood disorders". Nat. Rev. Neurosci. 11 (9): 642–51. doi:10.1038/nrn2884. PMID 20717121.