Health insurance in the United States
In the United States, health insurance is any program that helps pay for medical expenses, whether through privately purchased insurance, social insurance or a social welfare program funded by the government.[1] Synonyms for this usage include "health coverage," "health care coverage" and "health benefits."
In a more technical sense, the term is used to describe any form of insurance that provides protection against the costs of medical services. This usage includes private insurance and social insurance programs such as Medicare, which pools resources and spreads the financial risk associated with major medical expenses across the entire population to protect everyone, as well as social welfare programs such as Medicaid and the State Children's Health Insurance Program, which provide assistance to people who cannot afford health coverage.
In addition to medical expense insurance, "health insurance" may also refer to insurance covering disability or long-term nursing or custodial care needs. Different health insurance provides different levels of financial protection and the scope of coverage can vary widely, with more than 40 percent of insured individuals reporting that their plans do not adequately meet their needs as of 2007.[2]
The share of Americans with health insurance has been steadily declining since at least 2000. As of 2010 just under 84% of Americans had some form of health insurance, which meant that more than 49 million people went without coverage for at least part of the year. Declining rates of coverage and underinsurance are largely attributable to rising insurance costs and high unemployment. As the pool of people with private health insurance has shrunk, Americans are increasingly reliant on public insurance. Public programs now cover 31% of the population and are responsible for 44% of health care spending. Public insurance programs tend to cover more vulnerable people with greater health care needs. Many of the reforms instituted by the Affordable Care Act of 2010 were designed to extend health care coverage to those without it.[3]
Enrollment and the Uninsured

According to the United States Census Bureau, roughly 55% obtain insurance through an employer, while about 10% purchase it directly. About 31% of Americans were enrolled in a public health insurance program: 14.5% (45 million – although that number has since risen to 48 million) had Medicare, 15.9% (49 million) had Medicaid, and 4.2% (13 million) had military health insurance (there is some overlap, causing percentages to add up to more than 100%).[3] Employers may also provide reimbursement for health insurance purchased individually by their employees through a Defined contribution health benefits plan. Employers are allowed to pay employees cash in lieu of health insurance, but this is uncommon as it is subject to strict IRS regulations.[4]
Trends in private coverage
The percentage of non-elderly workers with employer-sponsored coverage has been falling, from 68% in 2000 to 61% in 2009, the latest year for which data is available.[5] While the primary cause of falling rates of insurance is the rising cost of health care for employers,[6] the economic downturn since 2008 has swelled the ranks of the uninsured, in large part because workers who lose their jobs also lose employer-sponsored insurance.[7] Over 1 million workers lost their health care coverage in January, February and March 2009. Approximately, 268,400 more workers lost health care coverage in March 2009 than in March 2008,[8] so the decline of employer sponsored insurance has likely accelerated in recent years.
Industry experts expect that in the coming decade there will be a shift to defined contribution health benefits plans, similar to the recent shift in retirement plans from defined benefit to defined contribution.[9][10]
Trends in public coverage
As a smaller and smaller share of the public is covered by private insurance, public insurance has grown more essential. In 2000, 10.5% of the public was covered by Medicaid, while 13.5% had Medicare. By 2010, those figures had risen to 14.5% and 15.9% respectively.[3]
A report published by the Kaiser Family Foundation in April 2008 found that economic downturns dramatically increase the public's reliance on state Medicaid and SCHIP and can cause significant financial strain for the programs. The authors estimated that a 1% increase in the unemployment rate would increase Medicaid and SCHIP enrollment by 1 million, and increase the number uninsured by 1.1 million. State spending on Medicaid and SCHIP would increase by $1.4 billion (total spending on these programs would increase by $3.4 billion). This increased spending would occur at the same time state government revenues were declining. During the last downturn, the Jobs and Growth Tax Relief Reconciliation Act of 2003 (JGTRRA) included federal assistance to states, which helped states avoid tightening their Medicaid and SCHIP eligibility rules. The authors conclude that Congress should consider similar relief for the current economic downturn.[11] Funding for Medicaid and SCHIP was in fact expanded significantly under the 2010 health reform bill.[12]
Status of the uninsured
.JPG)
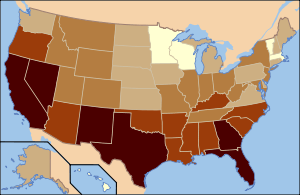
Based on self-reported census data, in 2010, more than 49 million people in the US (more than 16% of the population) were without health insurance as defined in the questions asked. The percentage of the non-elderly population who are uninsured has been generally increasing since the year 2000.[6] Among the uninsured population, some 40 million were employment-age adults (ages 18 to 64), and more than 28 million worked at least part-time. About 37% of the uninsured live in households with incomes over $50,000.[3]
According to the Census Bureau, more than 40 million of the uninsured are US citizens. Another 9.7 million are non-citizens, but the Census Bureau does not distinguish in its estimate between documented and undocumented migrants.[3] It has been estimated that nearly one fifth of the uninsured population is able to afford insurance, almost one quarter is eligible for public coverage, and the remaining 56% need financial assistance (8.9% of all Americans).[13] An estimated 5 million of those without health insurance are considered "uninsurable" because of pre-existing conditions (No longer true - old source?).[14]
A 2011 study found that there were 2.1 million hospital stays for uninsured patients, accounting for 4.4 percent ($17.1 billion) of total aggregate inpatient hospital costs in the United States.[15] The costs of treating the uninsured must often be absorbed by providers as charity care, passed on to the insured via cost-shifting and higher health insurance premiums, or paid by taxpayers through higher taxes.[16]
Death
Since people who lack health insurance are unable to obtain timely medical care, they have a 40 percent higher risk of death in any given year than those with health insurance, according to a study published in the American Journal of Public Health. The study estimated that in 2005 in the United States, there were 45,000 deaths associated with lack of health insurance.[17] A 2008 systematic review found consistent evidence that health insurance increased utilization of services and improved health.[18]
A Johns Hopkins Hospital study found that heart transplant complications occurred most often amongst the uninsured, and that patients who had private health plans fared better than those covered by Medicaid or Medicare.[19] Gallup issued a report in July 2014 stating that the uninsured rate for adults 18 and over declined from 18% in 2013 to 13.4% by in 2014, largely due to new coverage options and market reforms under the Affordable Care Act.[20] Rand Corporation had similar findings.[21]
Reform
The Affordable Care Act of 2010 was designed primarily to extend health coverage to those without it by expanding Medicaid, creating financial incentives for employers to offer coverage, and requiring those without employer or public coverage to purchase insurance in newly created state-run health insurance exchanges. The CBO has estimated that roughly 33 million who would have otherwise been uninsured will receive coverage because of the act by 2022.[22]
History
Accident insurance was first offered in the United States by the Franklin Health Assurance Company of Massachusetts. This firm, founded in 1850, offered insurance against injuries arising from railroad and steamboat accidents. Sixty organizations were offering accident insurance in the US by 1866, but the industry consolidated rapidly soon thereafter. While there were earlier experiments, the origins of sickness coverage in the US effectively date from 1890. The first employer-sponsored group disability policy was issued in 1911, but this plan's primary purpose was replacing wages lost due to an inability to work, not medical expenses.[23]
Before the development of medical expense insurance, patients were expected to pay all other health care costs out of their own pockets, under what is known as the fee-for-service business model. During the middle to late 20th century, traditional disability insurance evolved into modern health insurance programs. Today, most comprehensive private health insurance programs cover the cost of routine, preventive, and emergency health care procedures, and also most prescription drugs, but this was not always the case. The rise of private insurance was accompanied by the gradual expansion of public insurance programs for those who could not acquire coverage through the market.
Hospital and medical expense policies were introduced during the first half of the 20th century. During the 1920s, individual hospitals began offering services to individuals on a pre-paid basis, eventually leading to the development of Blue Cross organizations in the 1930s.[23] The first employer-sponsored hospitalization plan was created by teachers in Dallas, Texas in 1929.[24] Because the plan only covered members' expenses at a single hospital, it is also the forerunner of today's health maintenance organizations (HMOs).[24][25][26]
In the 1930s, The Roosevelt Administration explored possibilities for creating a national health insurance program, while it was designing the Social Security system. But it abandoned the project because the American Medical Association (AMA) fiercely opposed it, along with all forms of health insurance at that time.[27]
The rise of employer-sponsored coverage
Employer-sponsored health insurance plans dramatically expanded as a direct result of wage controls imposed by the federal government during World War II.[24] The labor market was tight because of the increased demand for goods and decreased supply of workers during the war. Federally imposed wage and price controls prohibited manufacturers and other employers from raising wages enough to attract workers. When the War Labor Board declared that fringe benefits, such as sick leave and health insurance, did not count as wages for the purpose of wage controls, employers responded with significantly increased offers of fringe benefits, especially health care coverage, to attract workers.[24]
President Harry S. Truman proposed a system of public health insurance in his November 19, 1945, address. He envisioned a national system that would be open to all Americans, but would remain optional. Participants would pay monthly fees into the plan, which would cover the cost of any and all medical expenses that arose in a time of need. The government would pay for the cost of services rendered by any doctor who chose to join the program. In addition, the insurance plan would give a cash balance to the policy holder to replace wages lost due to illness or injury. The proposal was quite popular with the public, but it was fiercely opposed by the Chamber of Commerce, the American Hospital Association, and the AMA, which denounced it as "socialism."[28]
Foreseeing a long and costly political battle, many labor unions chose to campaign for employer-sponsored coverage, which they saw as a less desirable but more achievable goal, and as coverage expanded the national insurance system lost political momentum and ultimately failed to pass. Using health care and other fringe benefits to attract the best employees, private sector, white-collar employers nationwide expanded the U.S. health care system. Public sector employers followed suit in an effort to compete. Between 1940 and 1960, the total number of people enrolled in health insurance plans grew seven-fold, from 20,662,000 to 142,334,000,[29] and by 1958, 75% of Americans had some form of health coverage.[30]
Kerr-Mills Act
Still, private insurance remained unaffordable or simply unavailable to many, including the poor, the unemployed, and the elderly. Before 1965, only half of seniors had health care coverage, and they paid three times as much as younger adults, despite having lower incomes.[31] Consequently, interest persisted in creating public health insurance for those left out of the private marketplace.
The 1960 Kerr-Mills Act provided matching funds to states assisting patients with their medical bills. In the early 1960s, Congress rejected a plan to subsidize private coverage for people with Social Security as unworkable, and an amendment to the Social Security Act creating a publicly run alternative was proposed. Finally, President Lyndon B. Johnson signed the Medicare and Medicaid programs into law in 1965, creating publicly run insurance for the elderly and the poor.[32] Medicare was later expanded to cover people with disabilities, end-stage renal disease, and ALS.
Towards universal coverage
Persistent lack of insurance among many working Americans continued to create pressure for a comprehensive national health insurance system. In the early 1970s, there was fierce debate between two alternative models for universal coverage. Senator Ted Kennedy proposed a universal single-payer system, while President Nixon countered with his own proposal based on mandates and incentives for employers to provide coverage while expanding publicly run coverage for low-wage workers and the unemployed. Compromise was never reached, and Nixon's resignation and a series of economic problems later in the decade diverted Congress's attention away from health reform.
Shortly after his inauguration, President Clinton offered a new proposal for a universal health insurance system. Like Nixon's plan, Clinton's relied on mandates, both for individuals and for insurers, along with subsidies for people who could not afford insurance. The bill would have also created "health-purchasing alliances" to pool risk among multiple businesses and large groups of individuals. The plan was staunchly opposed by the insurance industry and employers' groups and received only mild support from liberal groups, particularly unions, which preferred a single payer system. Ultimately it failed after the Republican takeover of Congress in 1994.[33]
Finally achieving universal health coverage remained a top priority among Democrats, and passing a health reform bill was one of the Obama Administration's top priorities. The Patient Protection and Affordable Care Act was similar to the Nixon and Clinton plans, mandating coverage, penalizing employers who failed to provide it, and creating mechanisms for people to pool risk and buy insurance collectively.[12] Earlier versions of the bill included a publicly run insurer that could compete to cover those without employer sponsored coverage (the so-called public option), but this was ultimately stripped to secure the support of moderates. The bill passed the Senate in December 2009 with all Democrats voting in favor and the House in March 2010 with the support of most Democrats. Not a single Republican voted in favor of it either time.
Public health care coverage
Public programs provide the primary source of coverage for most seniors and also low-income children and families who meet certain eligibility requirements. The primary public programs are Medicare, a federal social insurance program for seniors (generally persons aged 65 and over) and certain disabled individuals; Medicaid, funded jointly by the federal government and states but administered at the state level, which covers certain very low income children and their families; and SCHIP, also a federal-state partnership that serves certain children and families who do not qualify for Medicaid but who cannot afford private coverage. Other public programs include military health benefits provided through TRICARE and the Veterans Health Administration and benefits provided through the Indian Health Service. Some states have additional programs for low-income individuals.[34] In 2011, approximately 60 percent of stays were billed to Medicare and Medicaid—up from 52 percent in 1997.[35]
Medicare
In the United States, Medicare is a federal social insurance program that provides health insurance to people over the age of 65, individuals who become totally and permanently disabled, end stage renal disease (ESRD) patients, and people with ALS. Recent research has found that the health trends of previously uninsured adults, especially those with chronic health problems, improves once they enter the Medicare program.[36] Traditional Medicare requires considerable cost-sharing, but ninety percent of Medicare enrollees have some kind of supplemental insurance - either employer-sponsored or retiree coverage, Medicaid, or a private Medigap plan – that covers some or all of their cost-sharing.[37] With supplemental insurance, Medicare ensures that its enrollees have predictable, affordable health care costs regardless of unforeseen illness or injury.
As the population covered by Medicare grows, its costs are projected to rise from slightly over 3 percent of GDP to over 6 percent, contributing substantially to the federal budget deficit.[38] In 2011, Medicare was the primary payer for an estimated 15.3 million inpatient stays, representing 47.2 percent ($182.7 billion) of total aggregate inpatient hospital costs in the United States.[15] The Affordable Care Act took some steps to reduce Medicare spending, and various other proposals are circulating to reduce it further.
Medicare Advantage
Medicare Advantage plans expand the health insurance options for people with Medicare. Medicare Advantage was created under the Balanced Budget Act of 1997, with the intent to better control the rapid growth in Medicare spending, as well as to provide Medicare beneficiaries more choices. But on average, Medicare Advantage plans cost 12% more than traditional Medicare.[39] The ACA took steps to align payments to Medicare Advantage plans with the cost of traditional Medicare.
There is some evidence that Medicare Advantage plans select patients with low risk of incurring major medical expenses to maximize profits at the expense of traditional Medicare.[40]
Medicare Part D
Medicare Part D provides a private insurance option to allow Medicare beneficiaries to purchase subsidized coverage for the costs of prescription drugs. It was enacted as part of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) and went into effect on January 1, 2006.[41]
Medicaid
Medicaid was instituted for the very poor in 1965. Since enrollees must pass a means test, Medicaid is a social welfare or social protection program rather than a social insurance program. Despite its establishment, the percentage of US residents who lack any form of health insurance has increased since 1994.[42] It has been reported that the number of physicians accepting Medicaid has decreased in recent years due to lower reimbursement rates.[43]
The Affordable Care Act dramatically expanded Medicaid. The program will now cover everyone with incomes under 133% of the federal poverty level who does not qualify for Medicare, provided this expansion of coverage has been accepted by the state where the person resides. Meanwhile, Medicaid benefits must be the same as the essential benefit in the newly created state exchanges. The federal government will fully fund the expansion of Medicaid initially, with some of the financial responsibility gradually devolving back to the states by 2020.
In 2011, there were 7.6 million hospital stays billed to Medicaid, representing 15.6% (approximately $60.2 billion) of total aggregate inpatient hospital costs in the United States.[15]
State Children's Health Insurance Program (SCHIP)
The State Children's Health Insurance Program (SCHIP) is a joint state/federal program to provide health insurance to children in families who earn too much money to qualify for Medicaid, yet cannot afford to buy private insurance. The statutory authority for SCHIP is under title XXI of the Social Security Act. SCHIP programs are run by the individual states according to requirements set by the federal Centers for Medicare and Medicaid Services, and may be structured as independent programs separate from Medicaid (separate child health programs), as expansions of their Medicaid programs (SCHIP Medicaid expansion programs), or combine these approaches (SCHIP combination programs). States receive enhanced federal funds for their SCHIP programs at a rate above the regular Medicaid match.
Military health benefits
Health benefits are provided to active duty service members, retired service members and their dependents by the Department of Defense Military Health System (MHS). The MHS consists of a direct care network of Military Treatment Facilities and a purchased care network known as TRICARE. Additionally, veterans may also be eligible for benefits through the Veterans Health Administration.
Indian health service
The Indian Health Service (IHS) provides medical assistance to eligible American Indians at IHS facilities, and helps pay the cost of some services provided by non-IHS health care providers.[34]
State risk pools
In 1976, some states began providing guaranteed-issuance risk pools, which enable individuals who are medically uninsurable through private health insurance to purchase a state-sponsored health insurance plan, usually at higher cost. Minnesota was the first to offer such a plan; 34 states (Alabama, Alaska, Arkansas, California, Colorado, Connecticut, Florida, Illinois, Indiana, Iowa, Kansas, Kentucky, Louisiana, Maryland, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, North Carolina, North Dakota, Oklahoma, Oregon, South Carolina, South Dakota, Tennessee, Texas, Utah, Washington, West Virginia, Wisconsin, Wyoming) now offer them. Plans vary greatly from state to state, both in their costs and benefits to consumers and in their methods of funding and operations. They serve a very small portion of the uninsurable market—about 182,000 people in the U.S. as of 2004,[44] and about 200,000 in 2008.[45]
These risk pools allow people with pre-existing conditions such as cancer, diabetes, heart disease or other chronic illnesses to be able to switch jobs or seek self-employment without fear of being without health care benefits.[46] However, the plans are expensive, with premiums that can be double the average policy, and the pools currently cover only 1 in 25 of the so-called "uninsurable" population.[14] Additionally, even plans which are not expensive can leave those enrolled with little real health insurance beyond "catastrophic" insurance; for example, one insurance plan through Minnesota's high-risk pool, while costing only $215 per quarter, includes a $10,000 deductible with no preventative or other health care covered unless and until the enrollee has spent $10,000 of their own money during the year on health care.[47] Very sick people can accumulate large medical bills during mandatory waiting periods before their medical expenses are covered, and there are often lifetime expenditure caps (maximums), after which the risk pool no longer pays for any medical expenses.[48]
Efforts to pass a national pool have been unsuccessful, but some federal tax money has been awarded to states to innovate and improve their plans. With the Patient Protection and Affordable Care Act, effective by 2014, it will be easier for people with pre-existing conditions to afford regular insurance, since all insurers will be fully prohibited from discriminating against or charging higher rates for any individuals based on pre-existing medical conditions.[49][50]
Pre-existing Condition Insurance Plan
The Pre-existing Condition Insurance Plan, or PCIP, is a transitional program created in the Patient Protection and Affordable Care Act (PPACA). Those eligible for PCIP are citizens of the United States or those legally residing in the U.S., who have been uninsured for the last 6 months and "have a pre-existing condition or have been denied health coverage because of their health condition." However, if one has health insurance or is enrolled in a state high risk pool, they are not eligible for PCIP, even if that coverage does not cover their medical condition. PCIP is run by the individual states or through the U.S. Department of Health and Human Services, which has a contract with the Government Employees Health Association, or GEHA, to administer benefits. Both will be funded by the federal government and provide three plan options. These options are the standard, extended, and the Health Savings Account option. PCIP only covers the individual enrollee and does not include family members or dependents. In 2014, the Affordable Care Act provision banning discrimination based on pre-existing conditions will be implemented and PCIP enrollees will be transitioned into new state-based health care exchanges.[51][52][53]
Private health care coverage
Private health insurance may be purchased on a group basis (e.g., by a firm to cover its employees) or purchased by individual consumers. Most Americans with private health insurance receive it through an employer-sponsored program. According to the United States Census Bureau, some 60% of Americans are covered through an employer, while about 9% purchase health insurance directly.[54] Private insurance was billed for 12.2 million inpatient hospital stays in 2011, incurring approximately 29% ($112.5 billion) of the total aggregate inpatient hospital costs in the United States.[15]
The US has a joint federal and state system for regulating insurance, with the federal government ceding primary responsibility to the states under the McCarran-Ferguson Act. States regulate the content of health insurance policies and often require coverage of specific types of medical services or health care providers.[55][56] State mandates generally do not apply to the health plans offered by large employers, due to the preemption clause of the Employee Retirement Income Security Act.
Employer sponsored
Employer-sponsored health insurance is paid for by businesses on behalf of their employees as part of an employee benefit package. Most private (non-government) health coverage in the US is employment-based. Nearly all large employers in America offer group health insurance to their employees.[57] The typical large-employer PPO plan is typically more generous than either Medicare or the Federal Employees Health Benefits Program Standard Option.[58]
The employer typically makes a substantial contribution towards the cost of coverage. Typically, employers pay about 85% of the insurance premium for their employees, and about 75% of the premium for their employees' dependents. The employee pays the remaining fraction of the premium, usually with pre-tax/tax-exempt earnings. These percentages have been stable since 1999.[59] Health benefits provided by employers are also tax-favored: Employee contributions can be made on a pre-tax basis if the employer offers the benefits through a section 125 cafeteria plan.
Although workers are effectively paid less than they would be, because of the cost of insurance premiums to the employer, employer-sponsored health insurance offers several benefits to workers, including economies of scale, a reduction in adverse selection pressures on the insurance pool (premiums are lower when all employees participate rather than just the sickest), and reduced income taxes.[24] The disadvantages include disruptions related to changing jobs, the regressive tax effect (high-income workers benefit far more from the tax exemption for premiums than low-income workers), and increased spending on healthcare.[24]
Costs for employer-paid health insurance are rising rapidly: since 2001, premiums for family coverage have increased 78%, while wages have risen 19% and inflation has risen 17%, according to a 2007 study by the Kaiser Family Foundation.[60] Employer costs have risen noticeably per hour worked, and vary significantly. In particular, average employer costs for health benefits vary by firm size and occupation. The cost per hour of health benefits is generally higher for workers in higher-wage occupations, but represent a smaller percentage of payroll.[61] The percentage of total compensation devoted to health benefits has been rising since the 1960s.[62] Average premiums, including both the employer and employee portions, were $4,704 for single coverage and $12,680 for family coverage in 2008.[59][63]
However, in a 2007 analysis, the Employee Benefit Research Institute concluded that the availability of employment-based health benefits for active workers in the US is stable. The "take-up rate," or percentage of eligible workers participating in employer-sponsored plans, has fallen somewhat, but not sharply. EBRI interviewed employers for the study, and found that others might follow if a major employer discontinued health benefits. Effective by January 1, 2014, the Patient Protection and Affordable Care Act will impose a $2000 per employee tax penalty on employers with over 50 employees who do not offer health insurance to their full-time workers. (In 2008, over 95% of employers with at least 50 employees offered health insurance.[64])[65] On the other hand, public policy changes could also result in a reduction in employer support for employment-based health benefits.[66]
Although much more likely to offer retiree health benefits than small firms, the percentage of large firms offering these benefits fell from 66% in 1988 to 34% in 2002.[57]
Small employer group coverage
According to a 2007 study, about 59% of employers at small firms (3-199 workers) in the US provide employee health insurance. The percentage of small firms offering coverage has been dropping steadily since 1999. The study notes that cost remains the main reason cited by small firms who do not offer health benefits.[67] Small firms that are new are less likely to offer coverage than ones that have been in existence for a number of years. For example, using 2005 data for firms with fewer than 10 employees, 43% of those that had been in existence at least 20 years offered coverage, but only 24% of those that had been in existence less than 5 years did. The volatility of offer rates from year to year also appears to be higher for newer small businesses.[68]
The types of coverage available to small employers are similar to those offered by large firms, but small businesses do not have the same options for financing their benefit plans. In particular, self-funded health care (whereby an employer provides health or disability benefits to employees with its own funds rather than contracting an insurance company[69]) is not a practical option for most small employers.[70] A RAND Corporation study published in April 2008 found that the cost of health care coverage places a greater burden on small firms, as a percentage of payroll, than on larger firms.[71] A study published by the American Enterprise Institute in August 2008 examined the effect of state benefit mandates on self-employed individuals, and found that "the larger the number of mandates in a state, the lower the probability that a self-employed person will be a significant employment generator."[72] Beneficiary cost sharing is, on average, higher among small firms than large firms.[73]
When small group plans are medically underwritten, employees are asked to provide health information about themselves and their covered family members when they apply for coverage. When determining rates, insurance companies use the medical information on these applications. Sometimes they will request additional information from an applicant's physician or ask the applicants for clarification.[74]
States regulate small group premium rates, typically by placing limits on the premium variation allowable between groups (rate bands). Insurers price to recover their costs over their entire book of small group business while abiding by state rating rules.[75] Over time, the effect of initial underwriting "wears off" as the cost of a group regresses towards the mean. Recent claim experience - whether better or worse than average - is a strong predictor of future costs in the near term. But the average health status of a particular small employer group tends to regress over time towards that of an average group.[76] The process used to price small group coverage changes when a state enacts small group reform laws.[77]
Insurance brokers play a significant role in helping small employers find health insurance, particularly in more competitive markets. Average small group commissions range from 2 percent to 8 percent of premiums. Brokers provide services beyond insurance sales, such as assisting with employee enrollment and helping to resolve benefits issues.[78]
College-sponsored health insurance for students
Many colleges, universities, graduate schools, professional schools and trade schools offer a school-sponsored health insurance plan. Many schools require that you enroll in the school-sponsored plan unless you are able to show that you have comparable coverage from another source.
Effective group health plan years beginning after September 23, 2010, if an employer-sponsored health plan allows employees' children to enroll in coverage, then the health plan must allow employees' adult children to enroll as well as long as the adult child is not yet age 26. Some group health insurance plans may also require that the adult child not be eligible for other group health insurance coverage, but only before 2014.[79]
This extension of coverage will help cover one in three young adults, according to White House documents.
Federal employees health benefit plan (FEHBP)
In addition to such public plans as Medicare and Medicaid, the federal government also sponsors a health benefit plan for federal employees—the Federal Employees Health Benefits Program (FEHBP). FEHBP provides health benefits to full-time civilian employees. Active-duty service members, retired service members and their dependents are covered through the Department of Defense Military Health System (MHS). FEHBP is managed by the federal Office of Personnel Management.
"Portability" of group coverage
Two federal laws address the ability of individuals with employment-based health insurance coverage to maintain coverage.
The Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) enables certain individuals with employer-sponsored coverage to extend their coverage if certain "qualifying events" would otherwise cause them to lose it. Employers may require COBRA-qualified individuals to pay the full cost of coverage, and coverage cannot be extended indefinitely. COBRA only applies to firms with 20 or more employees, although some states also have "mini-COBRA" laws that apply to small employers.
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) provides for forms of both "group-to-group" and "group-to-individual" portability. When an individual moves from one employer's benefit plan to another's, the new plan must count coverage under the old plan against any waiting period for pre-existing conditions, as long as there is not a break in coverage of more than 63 days between the two plans. When certain qualified individuals lose group coverage altogether, they must be guaranteed access to some form of individual coverage. To qualify, they must have at least 18 months of prior continuous coverage. The details of access and the price of coverage are determined on a state-by-state basis.
Association group health insurance
Regular health insurance is sometimes available to members of associations. Associations such as the American Bar Association offer health insurance to their members, using an established insurance company to write the policies for a group plan.[80]
Individually purchased
According to the US Census Bureau, about 9% of Americans are covered under health insurance purchased directly.[54] The range of products available is similar to those provided through employers. However, average out-of-pocket spending is higher in the individual market, with higher deductibles, co-payments and other cost-sharing provisions.[73][81] Major medical is the most commonly purchased form of individual health insurance. Although a major medical health insurance policy is primarily a catastrophic plan, qualified preventive benefits are still covered at 100% without any waiting period or copay.[82]
In the individual market, the consumer pays the entire premium without benefit of an employer contribution.[81][83] While self-employed individuals receive a tax deduction for their health insurance and can buy health insurance with additional tax benefits, most consumers in the individual market do not receive any tax benefit.[84]
Premiums vary significantly by age.[81][85][86] In states that allow individual medical plan underwriting, premiums also vary by health status.[81] However, with the Patient Protection and Affordable Care Act, effective by 2014, all insurers will be fully prohibited from discriminating against or charging higher rates for any individuals based on pre-existing medical conditions.[49][50]
In August 2008, the Hartford Courant reported that competition was increasing in the individual health insurance market, with more insurers entering the market, an increased variety of products, and a broader spread of prices.[87]
Individual health insurance is primarily regulated at the state level, consistent with the McCarran-Ferguson Act. Model acts and regulations promulgated by the National Association of Insurance Commissioners (NAIC) provide some degree of uniformity state to state. These models do not have the force of law and have no effect unless they are adopted by a state. They are, however, used as guides by most states, and some states adopt them with little or no change.
Types of medical insurance
Traditional indemnity or fee-for-service
Early hospital and medical plans offered by insurance companies paid either a fixed amount for specific diseases or medical procedures (schedule benefits) or a percentage of the provider's fee. The relationship between the patient and the medical provider was not changed. The patient received medical care and was responsible for paying the provider. If the service was covered by the policy, the insurance company was responsible for reimbursing or indemnifying the patient based on the provisions of the insurance contract ("reimbursement benefits"). Health insurance plans that are not based on a network of contracted providers, or that base payments on a percentage of provider charges, are still described as indemnity or fee-for-service plans.[23]
Blue Cross Blue Shield Association
The Blue Cross and Blue Shield Association (BCBSA) is a federation of 38 separate health insurance organizations and companies in the United States. Combined, they directly or indirectly provide health insurance to over 100 million Americans.[88] BCBSA insurance companies are franchisees, independent of the association (and traditionally each other), offering insurance plans within defined regions under one or both of the association's brands. Blue Cross Blue Shield insurers offer some form of health insurance coverage in every U.S. state. They also act as administrators of Medicare in many states or regions of the U.S., and provide coverage to state government employees as well as to the federal government employees under a nationwide option of the Federal Employees Health Benefit Plan.[89]
Health Maintenance Organizations
A health maintenance organization (HMO) is a type of managed care organization (MCO) that provides a form of health care coverage that is fulfilled through hospitals, doctors, and other providers with which the HMO has a contract. The Health Maintenance Organization Act of 1973 required employers with 25 or more employees to offer federally certified HMO options.[90] Unlike traditional indemnity insurance, an HMO covers only care rendered by those doctors and other professionals who have agreed to treat patients in accordance with the HMO's guidelines and restrictions in exchange for a steady stream of customers. Benefits are provided through a network of providers. Providers may be employees of the HMO ("staff model"), employees of a provider group that has contracted with the HMO ("group model"), or members of an independent practice association ("IPA model"). HMOs may also use a combination of these approaches ("network model").[23][91]
Managed care
The term managed care is used to describe a variety of techniques intended to reduce the cost of health benefits and improve the quality of care. It is also used to describe organizations that use these techniques ("managed care organization").[92] Many of these techniques were pioneered by HMOs, but they are now used in a wide variety of private health insurance programs. Through the 1990s, managed care grew from about 25% US employees with employer-sponsored coverage to the vast majority.[93]
| Year | Conventional plans | HMOs | PPOs | POS plans | HDHP/SOs |
|---|---|---|---|---|---|
| 1998 | 14% | 27% | 35% | 24% | ~ |
| 1999 | 10% | 28% | 39% | 24% | ~ |
| 2000 | 8% | 29% | 42% | 21% | ~ |
| 2001 | 7% | 24% | 46% | 23% | ~ |
| 2002 | 4% | 27% | 52% | 18% | ~ |
| 2003 | 5% | 24% | 54% | 17% | ~ |
| 2004 | 5% | 25% | 55% | 15% | ~ |
| 2005 | 3% | 21% | 61% | 15% | ~ |
| 2006 | 3% | 20% | 60% | 13% | 4% |
| 2007 | 3% | 21% | 57% | 15% | 5% |
| 2008 | 2% | 20% | 58% | 12% | 8% |
| 2009 | 1% | 20% | 60% | 10% | 8% |
| 2010 | 1% | 19% | 58% | 8% | 13% |
| 2011 | 1% | 17% | 55% | 10% | 17% |
| 2012 | <1% | 16% | 56% | 9% | 19% |
| 2013 | <1% | 14% | 57% | 9% | 20% |
Network-based managed care
Many managed care programs are based on a panel or network of contracted health care providers. Such programs typically include:
- A set of selected providers that furnish a comprehensive array of health care services to enrollees;
- Explicit standards for selecting providers;
- Formal utilization review and quality improvement programs;
- An emphasis on preventive care; and
- Financial incentives to encourage enrollees to use care efficiently.
Provider networks can be used to reduce costs by negotiating favorable fees from providers, selecting cost effective providers, and creating financial incentives for providers to practice more efficiently.[26] A survey issued in 2009 by America's Health Insurance Plans found that patients going to out-of-network providers are sometimes charged extremely high fees.[95][96]
Network-based plans may be either closed or open. With a closed network, enrollees' expenses are generally only covered when they go to network providers. Only limited services are covered outside the network—typically only emergency and out-of-area care. Most traditional HMOs were closed network plans. Open network plans provide some coverage when an enrollee uses non-network provider, generally at a lower benefit level to encourage the use of network providers. Most preferred provider organization plans are open-network (those that are not are often described as exclusive provider organizations, or EPOs), as are point of service (POS) plans.
The terms "open panel" and "closed panel" are sometimes used to describe which health care providers in a community have the opportunity to participate in a plan. In a "closed panel" HMO, the network providers are either HMO employees (staff model) or members of large group practices with which the HMO has a contract. In an "open panel" plan the HMO or PPO contracts with independent practitioners, opening participation in the network to any provider in the community that meets the plan's credential requirements and is willing to accept the terms of the plan's contract.
Other managed care techniques
Other managed care techniques include such elements as disease management, case management, wellness incentives, patient education, utilization management and utilization review. These techniques can be applied to both network-based benefit programs and benefit programs that are not based on a provider network. The use of managed care techniques without a provider network is sometimes described as "managed indemnity."
Blurring lines
Over time, the operations of many Blue Cross and Blue Shield operations have become more similar to those of commercial health insurance companies.[97] However, some Blue Cross and Blue Shield plans continue to serve as insurers of last resort.[98] Similarly, the benefits offered by Blues plans, commercial insurers, and HMOs are converging in many respects due to market pressures. One example is the convergence of preferred provider organization (PPO) plans offered by Blues and commercial insurers and the point of service plans offered by HMOs. Historically, commercial insurers, Blue Cross and Blue Shield plans, and HMOs might be subject to different regulatory oversight in a state (e.g., the Department of Insurance for insurance companies, versus the Department of Health for HMOs). Today, it is common for commercial insurance companies to have HMOs as subsidiaries, and for HMOs to have insurers as subsidiaries (the state license for an HMO is typically different from that for an insurance company).[23][91][99] At one time the distinctions between traditional indemnity insurance, HMOs and PPOs were very clear; today, it can be difficult to distinguish between the products offered by the various types of organization operating in the market.[100]
The blurring of distinctions between the different types of health care coverage can be seen in the history of the industry's trade associations. The two primary HMO trade associations were the Group Health Association of America and the American Managed Care and Review Association. After merging, they were known as American Association of Health Plans (AAHP). The primary trade association for commercial health insurers was the Health Insurance Association of America (HIAA). These two have now merged, and are known as America's Health Insurance Plans (AHIP).
New types of medical plans
In recent years, various new types of medical plans have been introduced.
- High-deductible health plan (HDHP)
Plans with much higher deductibles than traditional health plans – primarily providing coverage for catastrophic illness – have been introduced.[101] Because of the high deductible, these provide little coverage for everyday expenses – and thus have potentially high out-of-pocket expenses – but do cover major expenses. Couple with these are various forms of savings plans.
- Tax-preferenced health care spending account
Coupled with high-deductible plans are various tax-advantaged savings plans – funds (such as salary) can be placed in a savings plan, and then go to pay the out-of-pocket expenses. This approach to addressing increasing premiums is dubbed "consumer driven health care", and received a boost in 2003, when President George W. Bush signed into law the Medicare Prescription Drug, Improvement, and Modernization Act. The law created tax-deductible Health Savings Accounts (HSAs), untaxed private bank accounts for medical expenses, which can be established by those who already have health insurance. Withdrawals from HSAs are only penalized if the money is spent on non-medical items or services. Funds can be used to pay for qualified expenses, including doctor's fees, Medicare Parts A and B, and drugs, without being taxed.[102]
Consumers wishing to deposit pre-tax funds in an HSA must be enrolled in a high-deductible insurance plan (HDHP) with a number of restrictions on benefit design; in 2007, qualifying plans must have a minimum deductible of US$1,050. Currently, the minimum deductible has risen to $1.200 for individuals and $2,400 for families. HSAs enable healthier individuals to pay less for insurance and deposit money for their own future health care, dental and vision expenses.[103]
HSAs are one form of tax-preferenced health care spending accounts. Others include Flexible Spending Accounts (FSAs), Archer Medical Savings Accounts (MSAs), which have been superseded by the new HSAs (although existing MSAs are grandfathered), and Health Reimbursement Accounts (HRAs). These accounts are most commonly used as part of an employee health benefit package.[104] While there are currently no government-imposed limits to FSAs, legislation currently being reconciled between the House of Representatives and Senate would impose a cap of $2,500. While both the House and Senate bills would adjust the cap to inflation, approximately 7 million Americans who use their FSAs to cover out-of-pocket health care expenses greater than $2,500 would be forced to pay higher taxes and health care costs.
In July 2009, Save Flexible Spending Plans, a national grassroots advocacy organization, was formed to protect against the restricted use of FSAs in health care reform efforts, Save Flexible Spending Accounts is sponsored by the Employers Council on Flexible Compensation (ECFC), a non-profit organization "dedicated to the maintenance and expansion of the private employee benefits on a tax-advantaged basis".[105] ECFC members include companies such as WageWorks Inc., a benefits provider based in San Mateo, California.
Most FSA participants are middle income Americans, earning approximately $55,000 annually.[106] Individuals and families with chronic illnesses typically receive the most benefit from FSAs; even when insured, they incur annual out-of-pocket expenses averaging $4,398 .[107] Approximately 44 percent of Americans have one or more chronic conditions .[108]
- Limited benefit plan
Opposite to high-deductible plans are plans which provide limited benefits – up to a low level – have also been introduced. These limited medical benefit plans pay for routine care and do not pay for catastrophic care, they do not provide equivalent financial security to a major medical plan. Annual benefit limits can be as low as $2,000. Lifetime maximums can be very low as well.
- Discount medical card
One option that is becoming more popular is the discount medical card. These cards are not insurance policies, but provide access to discounts from participating health care providers. While some offer a degree of value, there are serious potential drawbacks for the consumer.[109]
- Short term
Short term health insurance plans have a short policy period (typically months) and are intended for people who only need insurance for a short time period before longer term insurance is obtained.[110] Short term plans typically cost less than traditional plans and have shorter application processes, but do not cover pre-existing conditions.
- Health care sharing
A Health care sharing ministry is an organization that facilitates sharing of health care costs between individual members who have common ethical or religious beliefs. Though a health care sharing ministry is not an insurance company, members are exempted from the individual responsibility requirements of the Patient Protection and Affordable Care Act.[111]
Health care markets and pricing
The US health insurance market is highly concentrated, as leading insurers have carried out over 400 mergers from the mid-1990s to the mid-2000s (decade). In 2000, the two largest health insurers (Aetna and UnitedHealth Group) had total membership of 32 million. By 2006 the top two insurers, WellPoint and UnitedHealth, had total membership of 67 million. The two companies together had more than 36% of the national market for commercial health insurance. The AMA has said that it "has long been concerned about the impact of consolidated markets on patient care." A 2007 AMA study found that in 299 of the 313 markets surveyed, one health plan accounted for at least 30% of the combined health maintenance organization (HMO)/preferred provider organization (PPO) market. In 90% of markets, the largest insurer controls at least 30% of the market, and the largest insurer controls more than 50% of the market in 54% of metropolitan areas.[112] The US Department of Justice has recognized this percentage of market control as conferring substantial monopsony power in the relations between insurer and physicians.[113]
Most provider markets (especially hospitals) are also highly concentrated, - roughly 80%, according to criteria established by the FTC and Department of Justice[114] - so insurers usually have little choice about which providers to include in their networks, and consequently little leverage to control the prices they pay. Large insurers frequently negotiate most-favored nation clauses with providers, agreeing to raise rates significantly while guaranteeing that providers will charge other insurers higher rates.[115]
According to some experts, such as Uwe Reinhardt,[116] Sherry Glied, Megan Laugensen,[117] Michael Porter, and Elizabeth Teisberg,[118] this pricing system is highly inefficient and is a major cause of rising health care costs. Health care costs in the United States vary enormously between plans and geographical regions, even when input costs are fairly similar, and rise very quickly. Health care costs have risen faster than economic growth at least since the 1970s. Public health insurance programs typically have more bargaining power as a result of their greater size and typically pay less for medical services than private plans, leading to slower cost growth, but the overall trend in health care prices have led public programs' costs to grow at a rapid pace as well.
Other types of health insurance (non-medical)
While the term "health insurance" is most commonly used by the public to describe coverage for medical expenses, the insurance industry uses the term more broadly to include other related forms of coverage, such as disability income and long-term care insurance.
Disability income insurance
Disability income (DI) insurance pays benefits to individuals who lose their ability to work due to injury or illness. DI insurance replaces income lost while the policyholder is unable to work during a period of disability (in contrast to medical expense insurance, which pays for the cost of medical care).[119] For most working age adults, the risk of disability is greater than the risk of premature death, and the resulting reduction in lifetime earnings can be significant. Private disability insurance is sold on both a group and an individual basis. Policies may be designed to cover long-term disabilities (LTD coverage) or short-term disabilities (STD coverage).[120] Business owners can also purchase disability overhead insurance to cover the overhead expenses of their business while they are unable to work.[121]
A basic level of disability income protection is provided through the Social Security Disability Insurance (SSDI) program for qualified workers who are totally and permanently disabled (the worker is incapable of engaging in any "substantial gainful work" and the disability is expected to last at least 12 months or result in death).
Long-term care insurance
Long-term care (LTC) insurance reimburses the policyholder for the cost of long-term or custodial care services designed to minimize or compensate for the loss of functioning due to age, disability or chronic illness.[122] LTC has many surface similarities to long-term disability insurance. There are at least two fundamental differences, however. LTC policies cover the cost of certain types of chronic care, while long-term-disability policies replace income lost while the policyholder is unable to work. For LTC, the event triggering benefits is the need for chronic care, while the triggering event for disability insurance is the inability to work.[119]
Private LTC insurance is growing in popularity in the US. Premiums have remained relatively stable in recent years. However, the coverage is quite expensive, especially when consumers wait until retirement age to purchase it. The average age of new purchasers was 61 in 2005, and has been dropping.[123]
Supplemental coverage
Private insurers offer a variety of supplemental coverages in both the group and individual markets. These are not designed to provide the primary source of medical or disability protection for an individual, but can assist with unexpected expenses and provide additional peace of mind for insureds. Supplemental coverages include Medicare supplement insurance, hospital indemnity insurance, dental insurance, vision insurance, accidental death and dismemberment insurance and specified disease insurance.[23]
Supplemental coverages are intended to:
- Supplement a primary medical expense plan by paying for expenses that are excluded or subject to the primary plan's cost-sharing requirements (e.g., co-payments, deductibles, etc.);
- Cover related expenses such as dental or vision care;
- Assist with additional expenses that may be associated with a serious illness or injury.[23]
Medicare Supplement Coverage (Medigap)
Medicare Supplement policies are designed to cover expenses not covered (or only partially covered) by the "original Medicare" (Parts A & B) fee-for-service benefits. They are only available to individuals enrolled in Medicare Parts A & B. Medigap plans may be purchased on a guaranteed issue basis (no health questions asked) during a six-month open enrollment period when an individual first becomes eligible for Medicare.[124] The benefits offered by Medigap plans are standardized.
Hospital indemnity insurance
Hospital indemnity insurance provides a fixed daily, weekly or monthly benefit while the insured is confined in a hospital. The payment is not dependent on actual hospital charges, and is most commonly expressed as a flat dollar amount. Hospital indemnity benefits are paid in addition to any other benefits that may be available, and are typically used to pay out-of-pocket and non-covered expenses associated with the primary medical plan, and to help with additional expenses (e.g., child care) incurred while in the hospital.[23][91]
Scheduled health insurance plans
Scheduled health insurance plans are an expanded form of Hospital Indemnity plans. In recent years, these plans have taken the name mini-med plans or association plans. These plans may provide benefits for hospitalization, surgical, and physician services. However, they are not meant to replace a traditional comprehensive health insurance plan. Scheduled health insurance plans are more of a basic policy providing access to day-to-day health care such as going to the doctor or getting a prescription drug, but these benefits will be limited and are not meant to be effective for catastrophic events. Payments are based upon the plan's "schedule of benefits" and are usually paid directly to the service provider. These plans cost much less than comprehensive health insurance. Annual benefit maximums for a typical scheduled health insurance plan may range from $1,000 to $25,000.[125]
Dental insurance
Dental insurance helps pay for the cost of necessary dental care. Few medical expense plans include coverage for dental expenses. About 97% of dental benefits in the United States is provided through separate policies from carriers—both stand-alone and medical affiliates—that specialize in this coverage. Typically, these dental plans offer comprehensive preventive benefits. However, major dental expenses, such as crowns and root canals, are just partially covered. Also, most carriers offer a lower rate if you select a plan that utilizes their Network providers. Discount dental programs are also available. These do not constitute insurance, but provide participants with access to discounted fees for dental work.
Vision care insurance
Vision care insurance provides coverage for routine eye care and is typically written to complement other medical benefits. Vision benefits are designed to encourage routine eye examinations and ensure that appropriate treatment is provided.[23]
Specified disease
Specified disease provides benefits for one or more specifically identified conditions. Benefits can be used to fill gaps in a primary medical plan, such as co-payments and deductibles, or to assist with additional expenses such as transportation and child care costs.[23]
Accidental death and dismemberment insurance
AD&D insurance is offered by group insurers and provides benefits in the event of accidental death. It also provides benefits for certain specified types of bodily injuries (e.g., loss of a limb or loss of sight) when they are the direct result of an accident.[23]
- Insurance companies have high administrative costs.[126] Private health insurers are a significant portion of the U.S. economy directly employing (in 2004) almost 470,000 people at an average salary of $61,409.[127]
- Health insurance companies are not actually providing traditional insurance, which involves the pooling of risk, because the vast majority of purchasers actually do face the harms that they are "insuring" against. Instead, as Edward Beiser and Jacob Appel have separately argued, health insurers are better thought of as low-risk money managers who pocket the interest on what are really long-term healthcare savings accounts.[128][129]
- According to a study by a pro-health reform group published February 11, the nation's largest five health insurance companies posted a 56 percent gain in 2009 profits over 2008. The insurers (Wellpoint, UnitedHealth, Cigna, Aetna and Humana) cover the majority of Americans with health insurance.[130]
See also
General:
- Health economics
- Insurance medicine
- National health insurance
- Public health
- Social welfare
- Universal health care
References
- ↑ See, for example, US Census Bureau,"CPS Health Insurance Definitions"
- ↑ Consumer Reports, "Are you really covered? Why 4 in 10 Americans can't depend on their health insurance." at the Wayback Machine (archived September 22, 2008) September 2007
- 1 2 3 4 5 "Income, Poverty, and Health Insurance Coverage in the United States: 2010." U.S. Census Bureau. Issued September 2011.
- ↑ Spilman Ingots, "Cash in Lieu of Health Insurance? Word to the Wise"
- ↑ Robert Wood Johnson Foundation and State Health Access Data Assistance Center, "State-Level Trends in Employer-Sponsored Health Insurance." June 2011
- 1 2 "Percentage of Nonelderly Americans Without Health Insurance Coverage, 1987-2006". CovertheUninsured.org, a project of the Robert Wood Johnson Foundation. Archived from the original on October 19, 2007. Retrieved January 21, 2008.
- ↑ "Changes in Health Insurance Coverage in the Great Recession, 2007-2010" John Holanan and Vicki Chen. Kaiser Family Foundation, December 2011
- ↑ "More Americans Losing Health Insurance Every Day". Americanprogress.org. Retrieved March 3, 2010.
- ↑ http://www.businessweek.com/news/2011-12-09/defined-contributions-define-health-care-future-peter-orszag.html
- ↑ http://www.bizjournals.com/atlanta/blog/a-healthy-conversation/2013/04/humana-ceo-health-insurance-will-go.html
- ↑ Stan Dorn, Bowen Garrett, John Holahan, and Aimee Williams, "Medicaid, SCHIP and Economic Downturn: Policy Challenges and Policy Responses," Kaiser Family Foundation, April 2008
- 1 2 Kaiser Family Foundation (April 15, 2011). "Summary of new health reform law" (PDF). Menlo Park, Calif.: Kaiser Family Foundation. Archived from the original (PDF) on April 17, 2012. Retrieved March 26, 2012.
- ↑ Dubay L, Holahan J and Cook A.,The Uninsured and the Affordability of Health Insurance Coverage, Health Affairs (Web Exclusive), November 2006. Accessed February 4, 2007.
- 1 2 Marcus, Aliza (May 7, 2008). "Baby Kendra's $300,000 Bill Pains Insurers, Inspires Candidates". Bloomberg News. Retrieved May 10, 2008.
- 1 2 3 4 Torio CM, Andrews RM. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2011. HCUP Statistical Brief #160. Agency for Healthcare Research and Quality, Rockville, MD. August 2013.
- ↑ The Cost of Lack of Health Insurance, American College of Physicians
- ↑ Park, Madison (September 18, 2009). "45,000 American deaths associated with lack of insurance". CNN. Retrieved February 19, 2015.
- ↑ Freeman, Joseph D.; Kadiyala, Srikanth; Bell, Janice F.; Martin, Diane P. (October 2008). "The Causal Effect of Health Insurance on Utilization and Outcomes in Adults". Medical Care. 46 (10): 1023–1032. doi:10.1097/MLR.0b013e318185c913.
- ↑ "Health Care System Flaws and Lack of Private Insurance Contribute To Higher Deaths Among Black Heart Transplant Patients." Johns Hopkins Hospital, May 31, 2010.
- ↑ In U.S., Uninsured Rate Sinks to 13.4% in Second Quarter-July 10, 2014
- ↑ Rand Corporation-Changes in Health Insurance Enrollment Since 2013
- ↑ Congressional Budget Office, "CBO and JCT's Estimates of the Effects of the Affordable Care Act on the Number of People Obtaining Employment-Based Health Insurance." March 2012
- 1 2 3 4 5 6 7 8 9 10 11 HIAA Insurance Education (1997). Fundamentals of health insurance, Part A. Washington, D.C.: Health Insurance Association of America. ISBN 1-879143-36-4.
- 1 2 3 4 5 6 Buchmueller, Thomas C.; Monheit, Alan C. (April 2009). "Employer-sponsored health insurance and the promise of health insurance reform. NBER Working Paper Number 14839" (PDF). Cambridge, Mass.: National Bureau of Economic Research. Retrieved March 24, 2010.
- ↑ O'Hare, Thomas P. (2000). Individual medical expense insurance. Bryn Mawr, Pa.: American College. p. 7. ISBN 1-57996-025-1.
- 1 2 HIAA Insurance Education (1995). Managed care: integrating the delivery and financing of health care. Washington, D.C.: Health Insurance Association of America. p. 9. ISBN 1-879143-26-7.
- ↑ Corning, Peter A. (1969). "Chapter 1: The First Round - 1912 to 1920". The evolution of Medicare: from idea to law. Washington, D.C.: Office of Research and Statistics, Social Security Administration. OCLC 25869. Retrieved March 26, 2012.
- ↑ Corning, Peter A. (1969). "Chapter 2: The Second Round - 1927 to 1940". The evolution of Medicare: from idea to law. Washington, D.C.: Office of Research and Statistics, Social Security Administration. OCLC 25869. Retrieved March 26, 2012.
- ↑ Thomasson, Melissa (April 17, 2003). Whaples, Robert, ed. "Health insurance in the United States". EH.Net Encyclopedia. Tucson, Ariz.: Economic History Association. Archived from the original on September 3, 2011. Retrieved August 21, 2011.
- ↑ Texas Association of Health Plans (June 2008). "Health insurance in Texas" (PDF). Austin, Tex.: Texas Association of Health Plans. pp. 2, 26. Archived from the original (PDF) on December 23, 2011. Retrieved August 21, 2011.
- ↑ NASI Study Panel on Medicare's Larger Social Role (February 1999). "Medicare and the American social contract" (PDF). Washington, D.C.: National Academy of Social Insurance. p. 2. Retrieved March 28, 2012.
- ↑ Corning, Peter A. (1969). "Chapter 3: The Third Round - 1943 to 1950". The evolution of Medicare: from idea to law. Washington, D.C.: Office of Research and Statistics, Social Security Administration. OCLC 25869. Retrieved March 26, 2012.
- ↑ Hoffman, Catherine (March 2009). "National health insurance—a brief history of reform efforts in the U.S." (PDF). Menlo Park, Calif.: Kaiser Family Foundation. Archived from the original (PDF) on May 24, 2012. Retrieved March 26, 2012.
- 1 2 U.S. Census Bureau, "CPS Health Insurance Definitions"
- ↑ Pfuntner A., Wier L.M., Elixhauser A. Overview of Hospital Stays in the United States, 2011. HCUP Statistical Brief #166. November 2013. Agency for Healthcare Research and Quality, Rockville, MD. .
- ↑ "In the Literature: Health of Previously Uninsured Adults After Acquiring Medicare Coverage," The Commonwealth Fund, December 2007
- ↑ "Kaiser Family Foundation. 2010 Medicare Chartbook", Figure 6.1
- ↑ "2011 Medicare Trustees Report"
- ↑ Brian Biles, Steve Guterman, and Emily Adrion, ""The Continuing Cost of Privatization: Extra Payments to Medicare Advantage."" The Commonwealth Fund, September 2008.
- ↑ Jason Brown, Mark Duggan, Ilyana Kuziemko, and William Woolston, ""How does Risk Selection Respond to Risk Adjustment? Evidence from the Medicare Advantage Program."" NBER Working Paper No. 16977, April 2011
- ↑ Overview
- ↑ Fronstin, P. "Sources of Health Insurance and Characteristics of the Uninsured: Analysis of the March 2007 Current Population Survey." Employee Benefit Research Institute Issue Briefs. 2007 Oct;(310):1-36
- ↑ Cunningham P, May J. "Medicaid patients increasingly concentrated among physicians." Track Rep. 2006 Aug;(16):1-5. PMID 16918046.
- ↑ State High-Risk Health Insurance Pool Participation, December 31, 2004, StateHealthFacts.org, 2004, accessed October 9, 2007
- ↑ "Health Insurance: Enrollment, Benefits, Funding, and Other Characteristics of State High-Risk Health Insurance Pools" (PDF). U.S. Government Accountability Office. July 22, 2009.
- ↑ Website of the National Association of State Comprehensive Health Insurance Plans (NASCHIP)
- ↑ Coverage Denied on YouTube
- ↑ Harold Pollack (February 18, 2010). "All together now: We need comprehensive reform". Washington Post.
- 1 2 Binckes, Jeremy; Nick Wing (March 22, 2010). "The Top 18 Immediate Effects Of The Health Care Bill". The Huffington Post. Retrieved March 22, 2010.
- 1 2 ALONSO-ZALDIVAR, Ricardo (March 24, 2010). "Gap in health care law's protection for children". Associated Press. Retrieved March 24, 2010.
- ↑ "Instructions for Completing Your Application for the Pre-Existing Condition Insurance Plan in 2011." National Finance Center. Issued November 2010.
- ↑ "Health Insurance Options in Arizona." Living With Diabetes.
- ↑ "Frequently asked questions." Pre-Existing Condition Insurance Plan.
- 1 2 "Income, Poverty, and Health Insurance Coverage in the United States: 2007." U.S. Census Bureau. Issued August 2008.
- ↑ Victoria Craig Bunce and JP Wieske, "Health Insurance Mandates in the States 2008", The Council for Affordable Health Insurance, 2008
- ↑ Michael J. New, "The Effect of State Regulations on Health Insurance Premiums: A Preliminary Analysis," The Heritage Center for Data Analysis, October 27, 2005
- 1 2 from the Centers for Medicare and Medicaid Services
- ↑ Dale Yamamoto, Tricia Neuman and Michelle Kitchman Strollo, How Does the Benefit Value of Medicare Compare to the Benefit Value of Typical Large Employer Plans?, Kaiser Family Foundation, September 2008
- 1 2 Gary Claxton, Jon R. Gabel, Bianca DiJulio, Jeremy Pickreign, Heidi Whitmore, Benjamin Finder, Marian Jarlenski, and Samantha Hawkins, "Employer Health Benefits: 2008," the Kaiser Family Foundation, September 2008, Exhibit 6.1, page 74
- ↑ "Health Insurance Premiums Rise 6.1 Percent In 2007, Less Rapidly Than In Recent Years But Still Faster Than Wages And Inflation" (Press release). Kaiser Family Foundation. September 11, 2007. Retrieved September 13, 2007.
- ↑ Paul Jacobs and Gary Claxton, "Employer Health Insurance Costs and Worker Compensation," Kaiser Family Foundation, March 2008
- ↑ Paul Jacobs, "Wages and Benefits: A Long-Term View," Kaiser Family Foundation, February 2008
- ↑ Gary Claxton, Jon R. Gabel, Bianca DiJulio, Jeremy Pickreign, Heidi Whitmore, Benjamin Finder, Marian Jarlenski, and Samantha Hawkins, "Health Benefits In 2008: Premiums Moderately Higher, While Enrollment In Consumer-Directed Plans Rises In Small Firms," Health Affairs, September 24, 2008
- ↑ Employer Health Benefits: 2008 Summary of Findings, Kaiser Family Foundation.
- ↑ Downey , Jamie (March 24, 2010). "Tax implications of health care reform legislation". Boston Globe. Retrieved March 25, 2010.
- ↑ Paul Fronstin, "The Future of Employment-Based Health Benefits: Have Employers Reached a Tipping Point?," The Employee Benefit Research Institute, EBRI Issue Brief No. 312, December 2007, www.ebri.org
- ↑ "Employer Health Benefits 2007 Annual Survey", Kaiser Family Foundation, National Opinion Research Center at University of Chicago, and Health Research and Educational Trust, accessed November 2007
- ↑ Paul Jacobs and Gary Claxton, "Offer Rates for Smaller Establishments by Business Age," Kaiser Family Foundation, May 2008
- ↑ About.com > What is a self-funded health plan? From Kelly Montgomery, former About.com Guide. Updated November 12, 2008
- ↑ Hannah Yoo, Karen Heath and Tom Wildsmith, "Small Group Health Insurance in 2006", America's Health Insurance Plans, September 2006
- ↑ Christine Eibner, The Economic Burden of Providing Health Insurance: How Much Worse Off Are Small Firms? Kauffman-RAND Institute for Entrepreneurship Public Policy, 2008 ISBN 978-0-8330-4411-2
- ↑ Aparna Mathur, "Health Insurance and Job Creation by the Self-Employed," American Enterprise Institute, August 22, 2008
- 1 2 John Bertko, Hannah Yoo and Jeff Lemieux, An Analysis of the Distribution of Cost-Sharing Levels in Individual and Small-Group Coverage, Policy Report, Changes in Health Care Financing & Organization (HCFO), Robert Wood Johnson Foundation, August 2009
- ↑ http://www.nahu.org/consumer/groupinsurance.cfm
- ↑ William R. Lane, "The Art & Science of Pricing Small Group Medical Coverage: Initial Pricing Schemes", Health Section News, Society of Actuaries, December 2000
- ↑ William R. Lane,"The Art & Science of Pricing Small Group Medical Coverage: Renewal Pricing", Health Section News, Society of Actuaries, April 2001
- ↑ Bill Lane, "The Art & Science of Pricing Small Group Medical Coverage: From Debits to Risk Factors," Health Section News, Society of Actuaries, April 2003
- ↑ Leslie Jackson Conwell,"The Role of Health Insurance Brokers: Providing Small Employers with a Helping Hand," Center for Studying Health System Change, Issue Brief No. 57, October 2002
- ↑ "Health care reform: Adult child coverage mandate". Reinhart Boerner Van Deuren SC. Lexology. May 26, 2010.
- ↑ Merrill Matthews,"Association Group Health Insurance Sparks Controversy" The Heartland Institute, Health Care News by Merrill Matthews, executive director of the Council or Affordable Health Insurance
- 1 2 3 4 Teresa Chovan, Hannah Yoo and Tom Wildsmith, "Individual Health Insurance: A Comprehensive Survey of Affordability, Access, and Benefits", America's Health Insurance Plans, August 2005
- ↑ "Individual Health Insurance: An Overview of Products," America's Health Insurance Plans (accessed July 28, 2008)
- ↑ Didem Bernard and Jessica Banthin, "Premiums in the Individual Health Insurance Market for Policyholders under Age 65: 2002 and 2005," Statistical Brief #202, Agency for Healthcare Research and Quality, April 2008
- ↑ "Update on Individual Health Insurance," Kaiser Family Foundation, August 2004, revised, page 5
- ↑ Risk Segmentation in the Individual Health Insurance Market. National Institutes of Health
- ↑ Elizabeth M. Tucker & Lindsey Hogan, "The Cost And Benefits Of Individual Health Insurance Plans: 2007," Forrester Research and EHealthInsurance, 2007
- ↑ Diane Levick, "More Health Insurers Competing In Individual Coverage Market," The Hartford Courant, August 18, 2008
- ↑ Blue Cross and Blue Shield Association — About Us
- ↑ United States Office of Personal Management, 2010 Nationwide Fee-for-Service Open to All
- ↑ Joseph L. Dorsey, "The Health Maintenance Organization Act of 1973(P.L. 93-222)and Prepaid Group Practice Plan," Medical Care, Vol. 13, No. 1, (Jan. 1975), pp. 1–9
- 1 2 3 HIAA Insurance Education (1992). Lynch, Margaret E., ed. Health insurance terminology: a glossary. Washington, D.C.: Health Insurance Association of America. ISBN 1-879143-13-5.
- ↑ Peter R. Koongstvedt, "The Managed Health Care Handbook," Fourth Edition, Aspen Publishers, Inc., 2001, p. 3 ISBN 0-8342-1726-0
- ↑ "Employer Health Insurance: 2007," Kaiser Family Foundation, September 2007
- ↑ "Employer Health Benefit Survey" (PDF). Kaiser Family Foundation. August 20, 2013.
- ↑ THE VALUE OF PROVIDER NETWORKS AND THE ROLE OF OUT-OF-NETWORK CHARGES IN RISING HEALTH CARE COSTS: A SURVEY OF CHARGES BILLED BY OUT-OF-NETWORK PHYSICIANS, America's Health Insurance Plans, August 2009
- ↑ Gina Kolata, "Survey Finds High Fees Common in Medical Care ," The New York Times, August 11, 2009
- ↑ Thomas P. O'Hare, "Individual Medical Expense Insurance," The American College, 2000, p. 14 ISBN 1-57996-025-1
- ↑ Blues plans provide open enrollment periods in MI, NC, PA and VA."Summary of Key Consumer Protections in Individual Health Insurance Markets", Georgetown University Health Policy Institute, 2004
- ↑ Managed Care: Integrating the Delivery and Financing of Health Care - Part B, Health Insurance Association of America, 1996, ISBN 1-879143-29-1
- ↑ Peter R. Koongstvedt, "The Managed Health Care Handbook," Fourth Edition, Aspen Publishers, Inc., 2001, p. 28 ISBN 0-8342-1726-0
- ↑ "Definition of High Deductible Health Plan". Retrieved November 2, 2015.
- ↑ "Health Savings Accounts FAQ". Retrieved December 5, 2010.
- ↑ Health Care Spending Accounts: What You Need to Know About HSAs, HRAs, FSAs, and MSAs, America's Health Insurance Plans, July 2005, accessed October 9, 2007
- ↑ "Comparison of Tax-Advantaged Health Care Spending Accounts," America's Health Insurance Plans, January 2005, http://www.ahipresearch.org/pdfs/ChartMSAFSAHRAHSAJan05.pdf
- ↑ Employee Council on Flexible Compensation
- ↑ Roll Call Save Flexible Spending Plans
- ↑ Johns Hopkins University, Partnership for Solutions 25 Medical Expenditure Panel Survey, 2001
- ↑ Anderson, G. Chronicle Conditions: Making the Case for Ongoing Care. Johns Hopkins University. November 2007. Americans have more than one chronic health problem The Almanac of Chronic Disease
- ↑ Mila Kofman, Jennifer Libster, and Eliza Bangit, "Discount Medical Cards: Innovation or Illusion?," Commonwealth Fund, March 2005
- ↑ Is Temporary Health Insurance Right for You?
- ↑ The Religious Alternative To Obamacare's Individual Mandate
- ↑ American Medical Association, "Competition in Health Insurance: A Comprehensive Study of U.S. Markets." February 2010.
- ↑ AMA (2007), Competition in health insurance: A comprehensive study of U.S. markets - 2007 update,
- ↑ Cory Capps and David Dranove, "Market concentration of hospitals." Bates White Economic Publications, July 2011.
- ↑ James F. Doherty and Monique Ras, "Most favored nation clauses in payer/provider agreements." Ohio Department of Insurance, Joint Legislative Study Commission on Most Favored Nation Clauses in Health Care Contracts
- ↑ Uwe Reinhardt, "The Many Different Prices Paid to Providers and the Flawed Theory of Cost Shifting: Is It Time For a More Rational All-Payer System?" Health Affairs, November 2011.
- ↑ Miriam J. Laugesen and Sherry A. Glied,""Higher Fees Paid to U.S. Physicians Drive Higher Spending for Physician Services Compared to Other Countries."" Health Affairs, September 2011
- ↑ Michael E. Porter and Elizabeth Olmsted Teisberg ""Redefining Competition in Healthcare."" Harvard Business Review, 2004
- 1 2 "Disability Income Insurance: A Primer," The Health Insurance Association of America, 2002, ISBN 1-879143-66-6
- ↑ "Disability Insurance: A Missing Piece in the Financial Security Puzzle," a chart book prepared by America's Health Insurance Plans and the Society of Actuaries' Disability Chart Book Task Force and funded by the Actuarial Foundation, October 2004
- ↑ Gary V. Powell, "Disability Income Insurance: Advanced Issues," The Health Insurance Association of America, 2003 ISBN 1-879143-73-9
- ↑ "Long-Term Care: Understanding Needs and Options," The Health Insurance Association of America, 2001, ISBN 1-879143-55-0
- ↑ "Who Buys Long‑Term Care Insurance? A 15‑Year Study of Buyers and Non‑Buyers, 1990‑2005," America's Health Insurance Plans, April 2007
- ↑ "Medigap – Medicare supplement insurance" medicareresources.org, March 5, 2015
- ↑ "Comprehensive Health Insurance vs. Scheduled Health Insurance"
- ↑ "Health insurance administrative costs eat up 20% of spending," Medical News Today, November 14, 2005
- ↑ "Health Insurance: Overview and Economic Impact in the States," America's Health Insurance Plans, November 2007
- ↑ Appel, Jacob M. Health "Insurance": A Criminal Enterprise
- ↑ Beiser, Edward. "The Emperor's New Scrubs," Medicine & Health RI, 1994
- ↑ Walker, Emily. ABC News. Health Insurers Post Record Profits: Insurance Firms Rake in Profits as They Cut Patients, Advocacy Group Says
External links
- Health Insurance | USA.gov
- Goodman, John C. (2008). "Health Insurance". In David R. Henderson (ed.). Concise Encyclopedia of Economics (2nd ed.). Indianapolis: Library of Economics and Liberty. ISBN 978-0865976658. OCLC 237794267.
- HEALTH INSURANCE QUOTES:Better Health Insurance Prices